
Basilar invagination, also called basilar impression, is a congenital or acquired craniocervical junction abnormality where the tip of the odontoid process projects above the foramen magnum.
On this page:
Terminology
The following terms are often used interchangeably because they describe upwards migration of the upper cervical spine, but they are not synonyms 7:
basilar invagination: congenital upward displacement of vertebral elements into a normal foramen magnum with normal bone
basilar impression: upward displacement of the dens due to acquired softening of bones at the base of skull
cranial settling: used instead of basilar impression in patients with rheumatoid arthritis; affects 5-10% 2,3
platybasia: skull base flattening that can present with basilar invagination
Epidemiology
Congenital basilar invagination may remain asymptomatic until the patient is an adult, most commonly in the second and third decades 7.
Associations
Approximately 30% (range 25-35%) of patients have associated neuraxis abnormalities 7:
Clinical presentation
Symptoms include weakness, neck pain, bowel and bladder disturbance and/or paresthesia 7.
Pathology
Basilar invagination may be congenital or acquired and is often associated with platybasia. There is stenosis of the foramen magnum and compression of the medulla oblongata resulting in neurological symptoms, obstructive hydrocephalus, syringomyelia or even death.
Etiology
Common causes can be recalled using the mnemonic PF ROACH.
Another approach is to divide them into congenital and acquired causes:
Congenital
clival or occipital condyle hypoplasia 7
atlas hypoplasia 7
Acquired
rickets 7
skull base infection 7
Types
Basilar invagination is divided into two groups based on the absence (group I) and presence (group II) of a Chiari malformation and can be of use in planning surgical management. Brainstem compression is due to odontoid process indentation in group I, while reduced posterior cranial fossa volume is the cause in group II 1.
Radiographic features
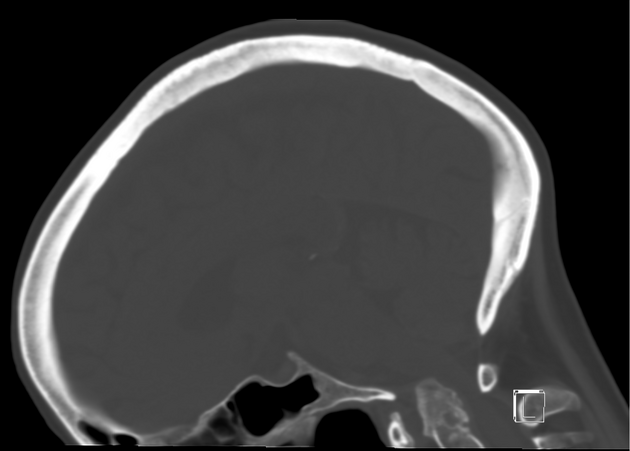
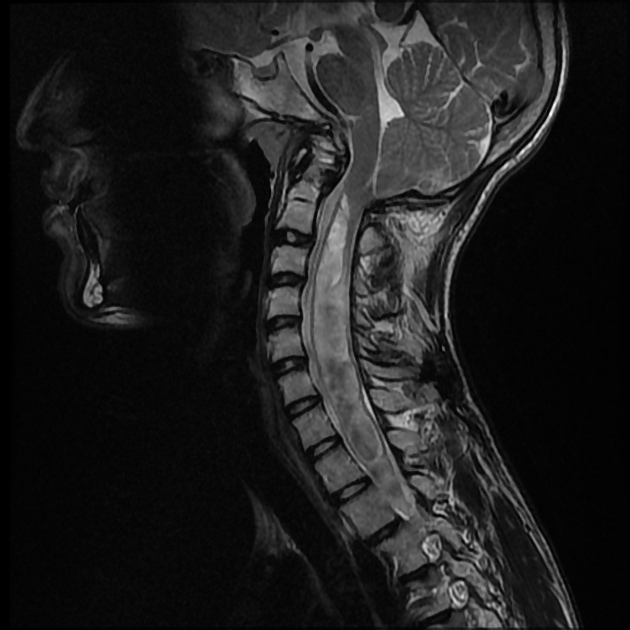
Five lines have been described and used by most radiologists to evaluate basilar invagination on frontal and lateral skull plain radiographs as well as coronal and midsagittal reconstructed CT and MRI images.
This is based on the relative projection of the odontoid process to these lines, which is as follows:
Frontal image
digastric line: the tip of the odontoid process is normally located 11 to 21 mm below this line
bimastoid line: the tip of the odontoid process projects normally not more than 10 mm above this line
Lateral image
-
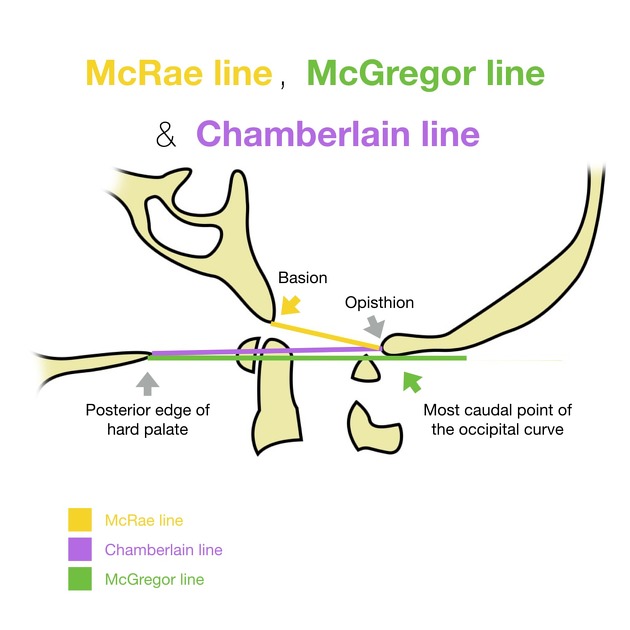
McRae line: connecting basion and opisthion
the tip of the odontoid process normally projects below this line, therefore, basilar invagination is diagnosed when the tip crosses this line
-
Chamberlain line: connecting the posterior border of hard palate and opisthion
the tip of the odontoid process projects normally not more than 3 mm above this line
-
McGregor line: connecting the posterior edge of the hard palate to the most caudal point of the occipital curve
the tip of the odontoid process projects normally not more than 5 mm above this line










 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.