
Craniopharyngioma (historical)
Citation, DOI, disclosures and article data
At the time the article was created Frank Gaillard had no recorded disclosures.
View Frank Gaillard's current disclosuresAt the time the article was last revised Henry Knipe had the following disclosures:
- Integral Diagnostics, Shareholder (ongoing)
- Micro-X Ltd, Shareholder (ongoing)
These were assessed during peer review and were determined to not be relevant to the changes that were made.
View Henry Knipe's current disclosures- Craniopharyngiomas
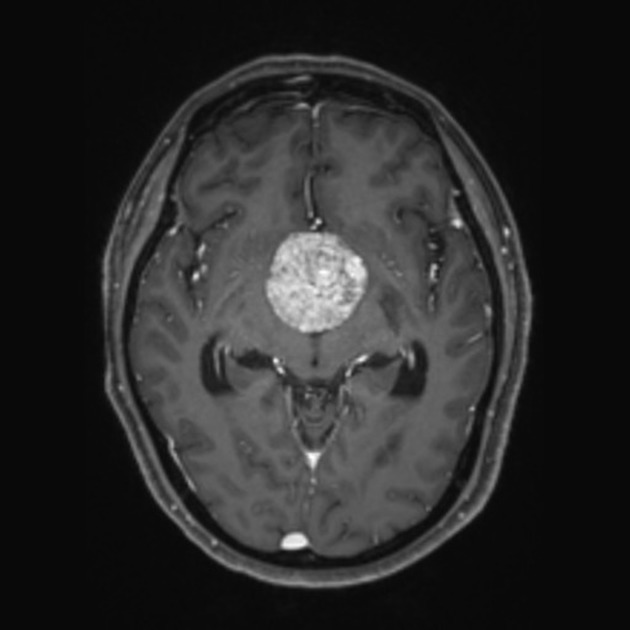
Craniopharyngioma is a term used to denote two separate entities (adamantinomatous craniopharyngiomas and papillary craniopharyngiomas), both relatively benign (WHO grade 1) neoplasms that typically arise in the sellar/suprasellar region.
Terminology
Until the 5th edition (2021) of the WHO classification of CNS tumors, adamantinomatous craniopharyngiomas and papillary craniopharyngiomas were considered subtypes of craniopharyngiomas 1.
Increasing molecular evidence has demonstrated that they have distinct and mutually exclusive mutations of CTNNB1 (adamantinomatous) and BRAF (papillary).
As such, they are now considered separate entities and will be discussed separately:
Quiz questions
References
- 1. Louis D, Perry A, Wesseling P et al. The 2021 WHO Classification of Tumors of the Central Nervous System: A Summary. Neuro Oncol. 2021;23(8):1231-51. doi:10.1093/neuonc/noab106 - Pubmed
Incoming Links
- Clival masses
- Lymphocytic hypophysitis
- Intracranial teratoma
- History of imaging of the pituitary region
- Pituitary lymphoma
- Extra-axial
- Optic canal enlargement
- Tumors of the base of skull (differential diagnosis)
- Pituitary stalk abnormal enhancement (differential)
- Pituitary xanthomatous lesions
- Ameloblastoma
- Intraventricular masses (an approach)
- Cavernous sinus syndrome
- Pituitary macroadenoma
- Intracranial epidermoid cyst
- Foster Kennedy syndrome
- Ectopic posterior pituitary
- Delayed bone age
- Pituitary metastasis
- Intracranial dermoid cyst
- Adamantinomatous craniopharyngioma
- Craniopharyngioma
- Chordoma
- Pilocytic astrocytoma - suprasellar
- Adamantinomatous craniopharyngioma
- Pituitary macroadenoma
- Adamantinomatous craniopharyngioma
- Adamantinomatous craniopharyngioma
- Adamantinomatous craniopharyngioma
- Adamantinomatous craniopharyngioma
- Adamantinomatous craniopharyngioma
- Adamantinomatous craniopharyngioma
- Adamantinomatous craniopharyngioma
- Adamantinomatous craniopharyngioma
- Adamantinomatous craniopharyngioma
- Adamantinomatous craniopharyngioma
- Adamantinomatous craniopharyngioma
- Adamantinomatous craniopharyngioma
- Adamantinomatous craniopharyngioma
- Adamantinomatous craniopharyngioma
Related articles: Pituitary region masses
-
general reading[+][+]
- pituitary gland anatomy
- pituitary MRI - an approach
-
pituitary region masses
- most common pituitary region masses
- solid and enhancing pituitary region mass
- mixed cystic and solid pituitary region mass
- mostly/purely cystic pituitary region masses
- purely intrasellar pituitary mass
- pituitary region mass with intrinsic high T1 signal
- abnormal enhancement/bulkiness of the pituitary infundibulum
- enlarged sella turcica
- mnemonic: SATCHMO
- history of imaging the pituitary region
-
pathology
-
pituitary tumors
- pituitary adenoma (commonest in the adult population)[+][+]
- pituitary carcinoma
- pituitary lymphoma
- meningioma
- craniopharyngioma
- optic pathway glioma
- germinoma
- chordoma
- dermoid (CNS) / epidermoid / intracranial teratoma
- pituicytoma
- spindle cell oncocytomas
- pituitary metastases
- granular cell tumor of the pituitary (pituitary choristoma)
- pilocytic astrocytoma of the neurohypophysis (infundibuloma)
- cellular infiltrates[+][+]
- other lesions[+][+]
- anterior circulation berry aneurysm
- hamartoma (tuber cinereum hamartoma)
- Rathke cleft cyst
- intracranial lipoma
- sphenoid sinus mucocoele
- pituitary abscess
- pituitary stone
-
pituitary tumors



 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.