
The term dolichoectasia means dilated and elongated. It is used to characterize arteries that have shown a significant deterioration of their tunica intima (and occasionally the tunica media), weakening the vessel walls and causing the artery to elongate and distend.
On this page:
Epidemiology
Dolichoectasias are more common in males 2. With intracranial dolichoectasia, the incidence is estimated at ~3% (range 0.06-5.8%) 2.
Clinical presentation
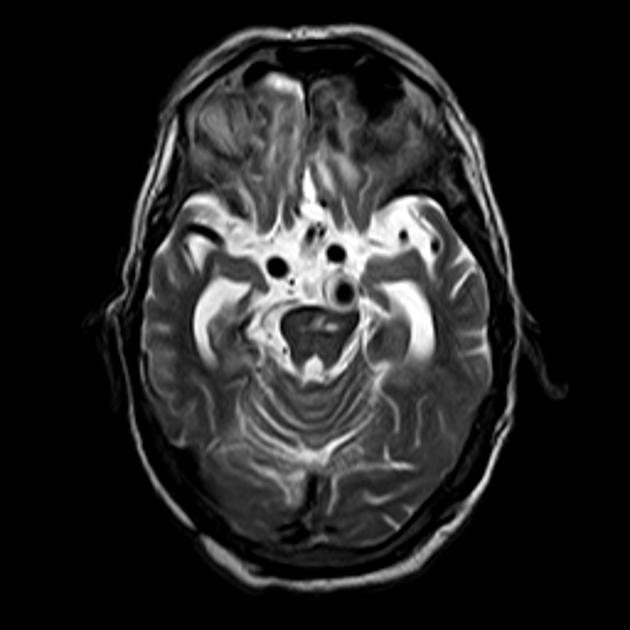
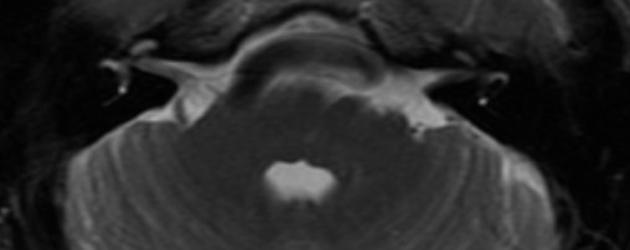
Ischemic effects on the brainstem and cerebellar hemispheres as well as symptoms related to hydrocephalus are common. Direct cranial nerve compression can lead to isolated cranial nerve dysfunction, usually associated with a normal-sized basilar artery that is tortuous and elongated (neurovascular compression syndrome (NVCS)). Cranial nerve dysfunction most commonly involves the cranial nerve VII and the cranial nerve V. Multiple cranial nerve dysfunction is far more likely to occur if there is dilation (ectasia) associated with a tortuous and elongated basilar artery. Cranial nerves affected in descending order of frequency include VII, V, III, VIII, and VI.
Pathology
As the arrangement of connective tissue is disturbed, the vessel wall is no longer able to hold its original conformation and begins to unravel due to the continued hypertension. High blood pressure molds and force the artery to take now on an elongated, tortuous course to better withstand the higher pressures.
Subtypes
Can be divided into several subtypes 3:
atherosclerotic dolichoectasia
non-atheroscerotic dolichoectasia
dolichoectatic appearance secondary to an arterial dissection
Etiology
Hypertension most commonly causes the atherosclerotic type. Continued stress on the walls of the artery will degrade the vessel wall by damaging and loosening the collagen and elastin meshwork that comprises the intima. Similarly, hypercholesterolemia or hyperlipidemia can also provide sufficient trauma to the vessel wall resulting in dolichoectasia.
Location
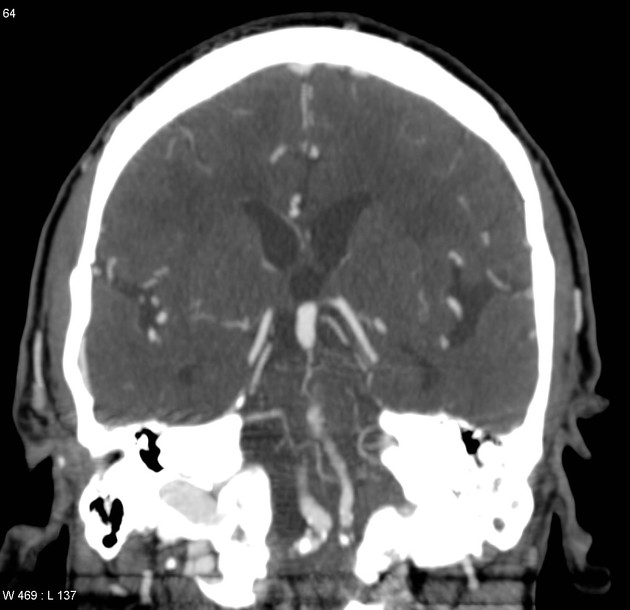
most commonly affected is the vertebrobasilar artery, see: vertebrobasilar dolichoectasia (VDBE)
internal carotid artery (ICA) is also at high risk to be affected
Associations
patients with autosomal dominant polycystic kidney disease (ADPKD), Marfan syndrome, and Ehlers-Danlos syndrome, are more likely to be subject to dolichoectasia(s) 9
dolichoectasia is also a characteristic finding in patients with Fabry disease10
Radiographic features
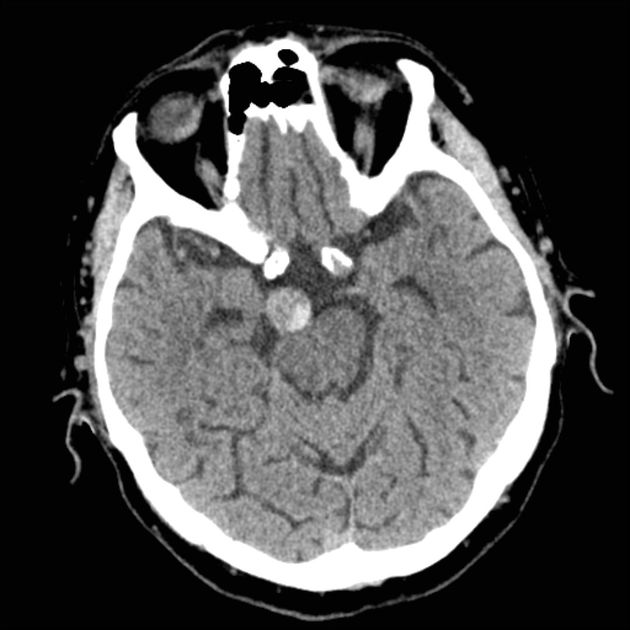
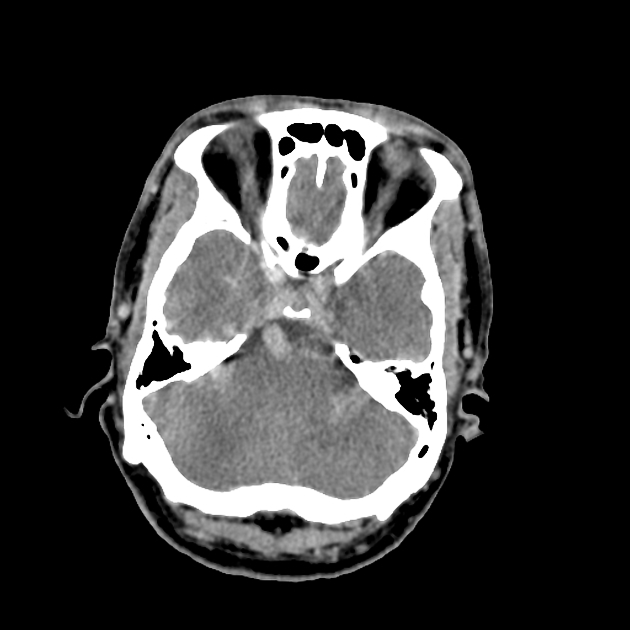
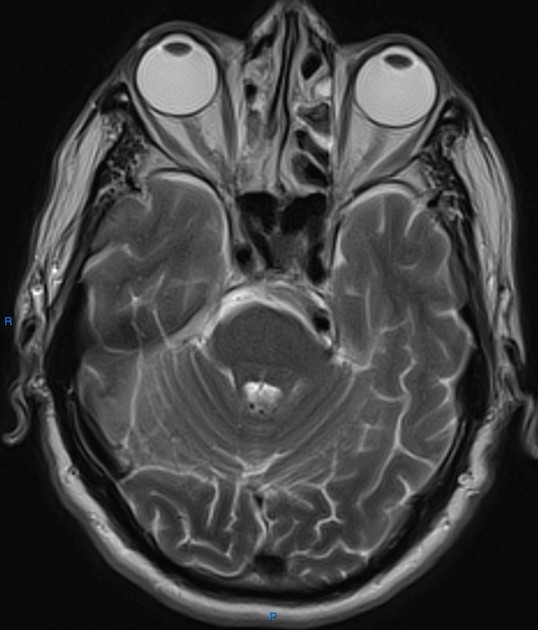
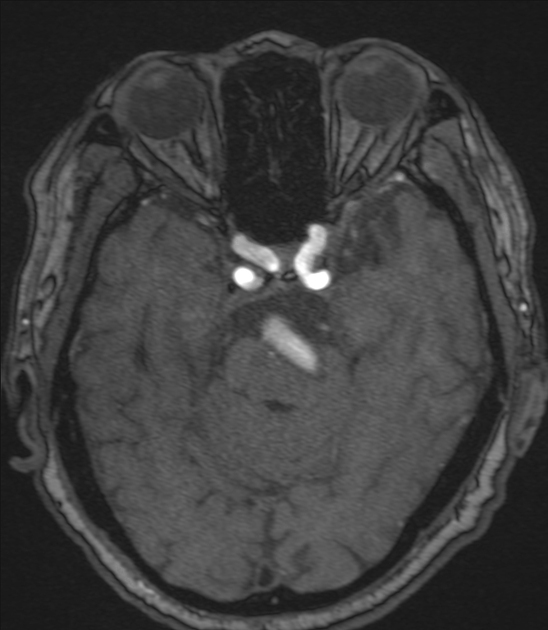
To be classified as dolichoectasia, in the vertebrobasilar system, the basilar arterial diameter should be >4.5 mm 1. Smoker's criteria uses three quantitative measures of basilar artery morphology: basilar artery diameter, laterality, and height of bifurcation 9.
Internal carotid artery dolichoectasia is particularly interesting because the artery typically already contains one hairpin turn. Seen in an MRI as two individual arteries at this hairpin, a carotid artery dolichoectasia can progress so far as to produce a second hairpin turn and appear as three individual arteries on an MRI. The pathogenesis is primarily related to compression of the optic nerves at the optic chiasma.
Treatment and prognosis
Treatment is limited with intervention restricted to symptomatic cases, although often this is difficult with limited options.
Complications
A systematic review of 375 patients determined a fairly high 5-year risk of complications 11:
brain infarction (17.6%)
brainstem compression (10.3%)
transient ischemic attack (10.1%)
hemorrhagic stroke (4.7%)
hydrocephalus (3.3%)
subarachnoid hemorrhage (2.6%)
The same review reported a 5-year mortality risk of 36.2%, with ischemic stroke as the most common cause of death 11.
Factors associated with adverse clinical outcomes include symptoms at the time of diagnosis, the severity of arterial dilation and dolichosis, mural T1 signal, mural thrombi, and interval ectasia progression on follow-up neuroimaging 11.





 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.