
Jugular paraganglioma (previously known as glomus jugulare) is a paraganglioma of the head and neck that is confined to the jugular fossa. While it is a rare tumor, it is the most common of the jugular fossa tumors.
On this page:
Terminology
The term "glomus" was historically used to describe certain types of neuroendocrine tumors arising from paraganglia. The term is, however, imprecise and can be confused with the glomus bodies and tumors that arise from them. It can also be mixed up with glomus tumors of the subcutaneous skin, also referred to as glomangioma.
Epidemiology
The relative prevalence of jugular paragangliomas with respect to other head and neck paraganglioma (e.g. tympanic paraganglioma and jugulotympanic paraganglioma) varies from publication to publication and depends on the definition of the terms jugular, tympanic, and jugulotympanic. Most agree however that they are more common than vagal paraganglioma 3.
These tumors are seen in adults, typically between 40 and 60 years of age, with a moderate female predilection 3.
Clinical presentation
Presentation depends on the degree of middle ear involvement. When significant involvement is present the lesion may cause pulsatile tinnitus and hearing loss.
Additionally, a number of patterns of cranial nerve palsies have been described due to the involvement of the nerves at the jugular foramen. These include 3-4:
Vernet syndrome (motor paralysis of cranial nerves IX, X, and XI)
Collet-Sicard syndrome (Vernet syndrome with additional involvement of cranial nerve XII)
Pathology
For a general discussion on the pathology of these tumors please refer to the generic article pertaining to paragangliomas.
Jugular tumors are defined according to the location (i.e. origin at the jugular foramen) rather than the anatomic origin and may arise from Jacobson nerve, Arnold nerve, or the jugular bulb 3.
Tumors may be bilateral, and other tumors such as carotid body tumors may coexist. Up to 10% of the patients may have multiple lesions. Tumors are locally infiltrating, and may rarely metastasize 4.
Radiographic features
Growth of these tumors is in a number of directions, typically extending into the mastoid air-cells, middle ear, and Eustachian tube.
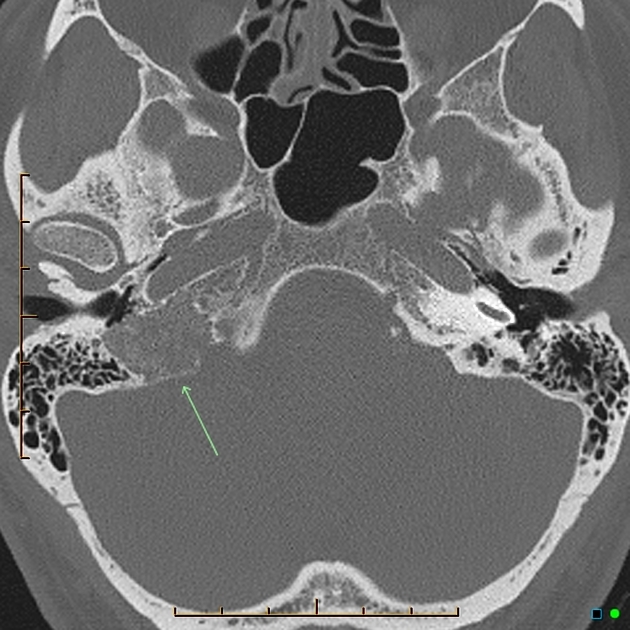
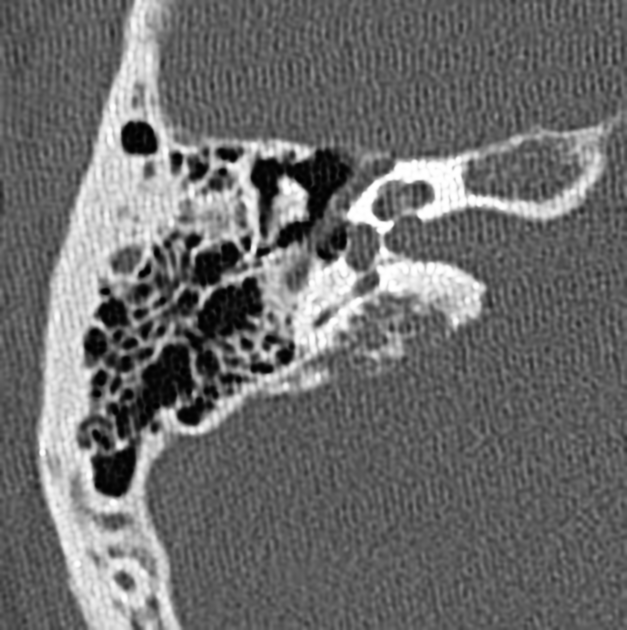
CT
CT is most useful at assessing the bony margins of the tumor, which are typically irregularly eroded with a moth-eaten pattern. Eventually, as the tumor enlarges the jugular spine is eroded and the mass extends into the middle ear, as well as inferiorly into the infratemporal fossa. CT is excellent at assessing the integrity of the ossicles and bony labyrinth 3. Also, erosion of the caroticojugular spine between the carotid canal and jugular fossa may be present (Phelp sign).
Angiography (DSA)
Angiography demonstrates an intense tumor blush, with the most common feeding vessel being the ascending pharyngeal 3. Early draining veins are also noted due to intra-tumoral shunting 4.
Angiography also has a role to play in preoperative embolization, which is typically carried out 1-2 days prior to surgery, however, care must be taken to fully evaluate feeding vessels. Familiarity with vascular anatomy of the region is essential if complications are to be avoided 3.
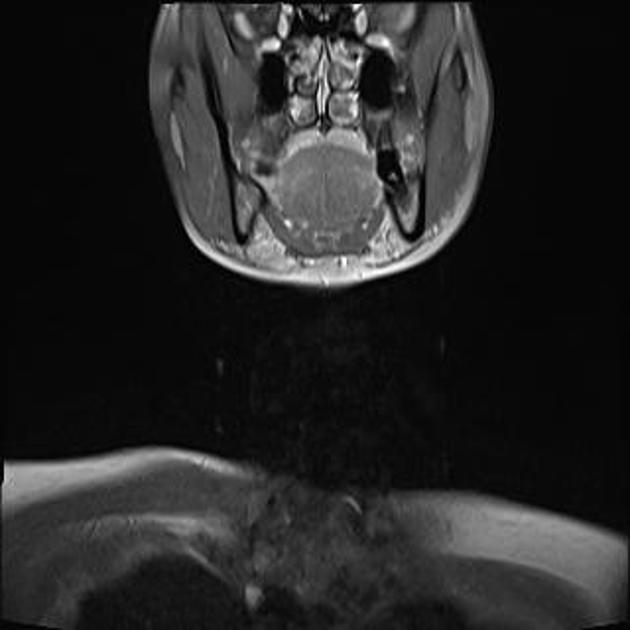
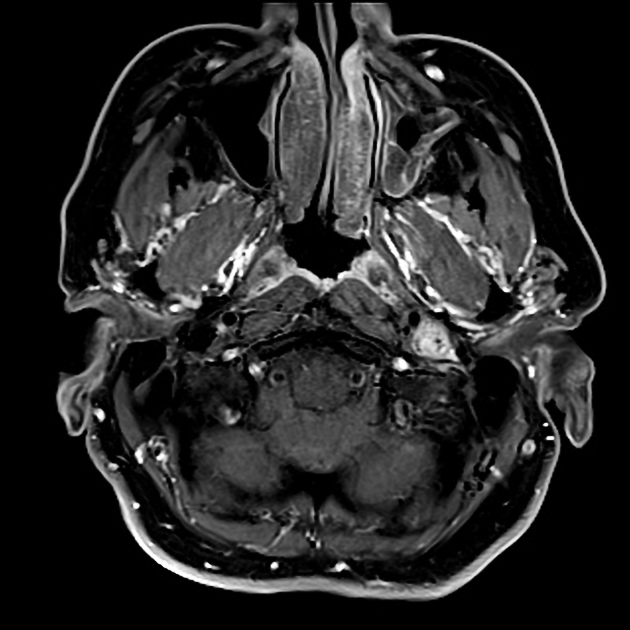
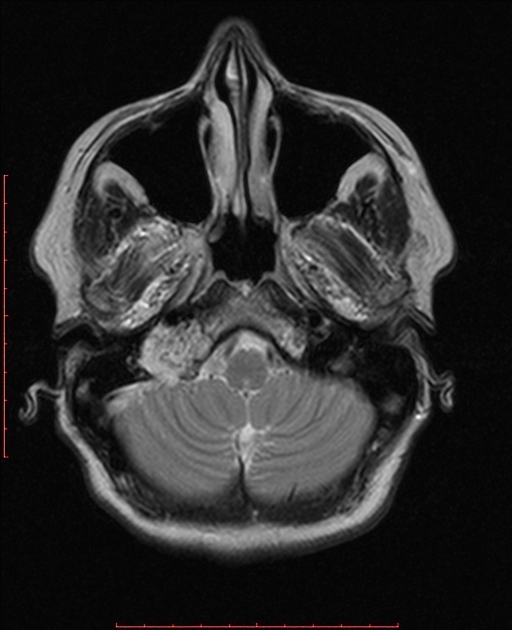
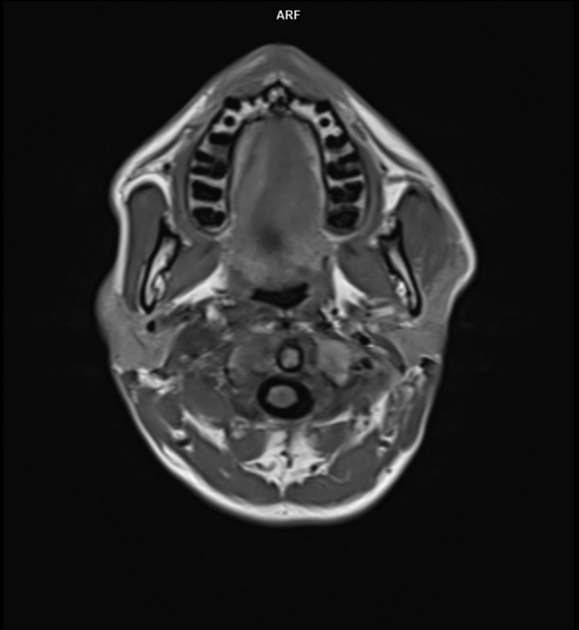
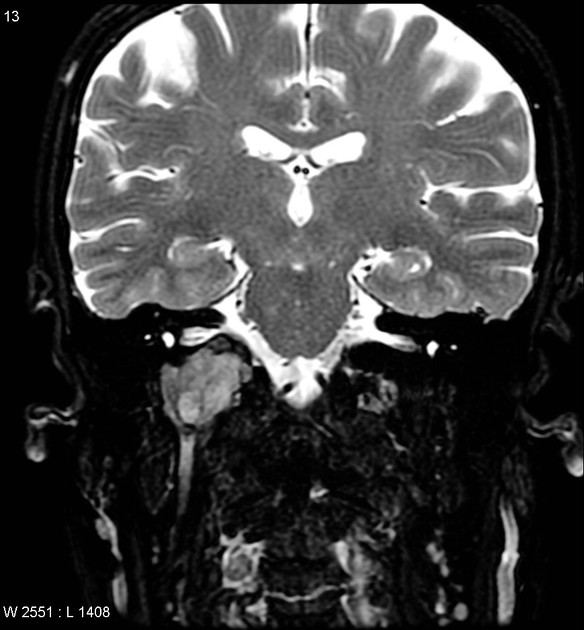
MRI
T1: low signal 3
T2: high signal
T1 C+ (Gd): marked intense enhancement 2-4
Salt and pepper appearance is seen on both T1 and T2 weighted sequences; the salt representing blood products from hemorrhage or slow flow and the pepper representing flow voids due to high vascularity. It should be noted that this appearance is sometimes encountered in other lesions (e.g. hypervascular metastases) and is not typically seen in smaller paragangliomas 3.
Nuclear medicine
Indium-111 labeled octreotide accumulates in these tumors due to the presence of receptors for somatostatin, best visualized with SPECT, but requires the tumor to be greater than 1.5 cm in diameter.
Treatment and prognosis
Surgery is the treatment of choice and if complete resection is achieved a cure can be expected.
Recurrence and local invasion are common, occurring in 40-50% of cases 3.
Although most cervical paragangliomas (e.g. carotid body tumors) are considered relatively radioresistant, the base of skull paragangliomas are radiosensitive, and thus large inoperable tumors or tumors in elderly and frail patients are often treated with radiotherapy.
Complications
Complications are not uncommon due to a large number of sensitive structures in the region and include:
CSF/endolymphatic leak
malignant transformation is less common, seen in 2-13% of cases 3.
Differential diagnosis
For a full list of differentials see the article on jugular fossa masses. General imaging differential considerations include:
-
sharply demarcated smooth bony margins 1
no internal flow voids
not very vascular on angiography
indium-111 labeled octreotide negative 3
-
bony metastases
hypervascular tumors may be very similar in appearances (e.g. renal cell carcinoma, thyroid cancer)
-
normal anatomical variation
asymmetry of jugular foraminal size
high riding or dehiscent jugular bulb
-
centered in the vestibular aqueduct rather than the jugular bulb




 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.