
Kommerell diverticula occur in some anomalies of the aortic arch system. It usually refers to the bulbous configuration of the origin of an aberrant left subclavian artery in the setting of a right-sided aortic arch. However, it was originally described as a diverticular outpouching at the origin of an aberrant right subclavian artery with a left-sided aortic arch and is also seen in aberrant right vertebral arteries (vertebral arteria lusoria).
On this page:
Epidemiology
The prevalence of aberrant right and left subclavian arteries is approximately 0.7-2% and 0.04-0.4% of the population respectively 10. in 20-60% of people with aberrant subclavian arteries are associated with Kommerell’s diverticulum 10.
Clinical presentation
Kommerell diverticulum may be asymptomatic or cause symptoms of esophageal or tracheal obstruction. Presentation in childhood can often be with airway symptoms whereas dysphagia and chest discomfort can be more common in the adult presentation.
Pathology
It is considered a developmental error with a remnant of the fourth dorsal aortic arch. Recent histological studies have suggested the presence of cystic medial necrosis in the diverticulum wall.
Radiographic features
Plain radiograph
On chest radiographs, a small rounded density may be seen laterally towards the left of the trachea.
Fluoroscopy
On a barium swallow, an impression can be seen from the left side of the esophagus simulating a double aortic arch.
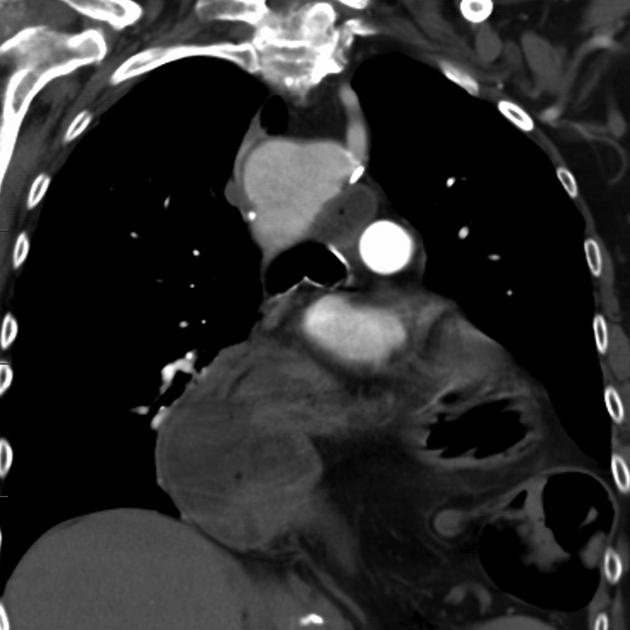
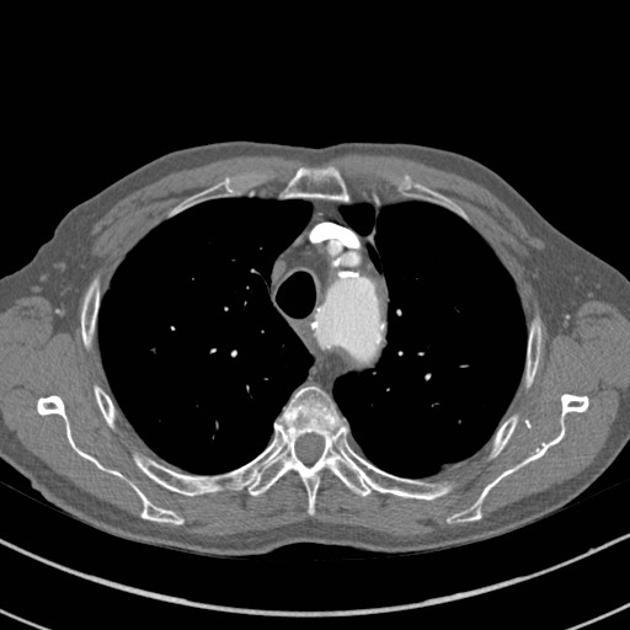
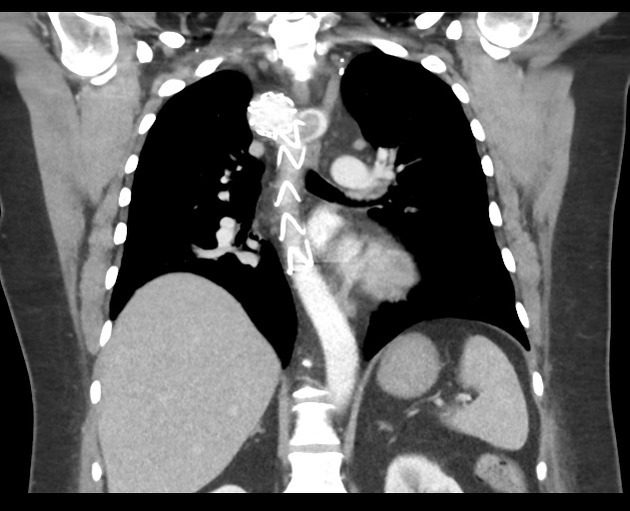
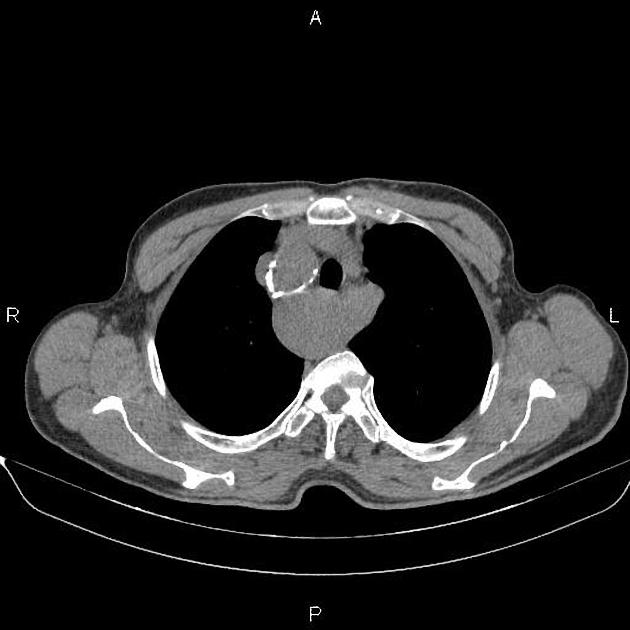
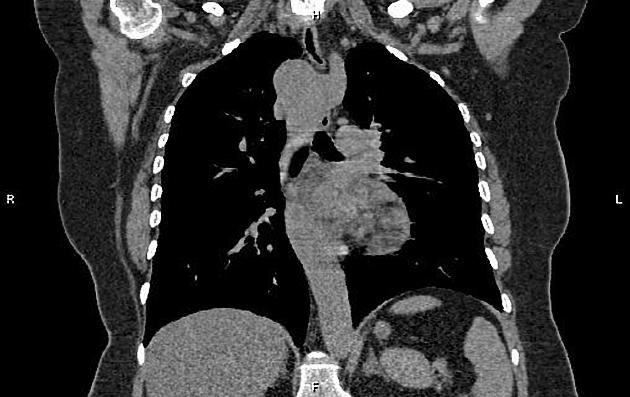
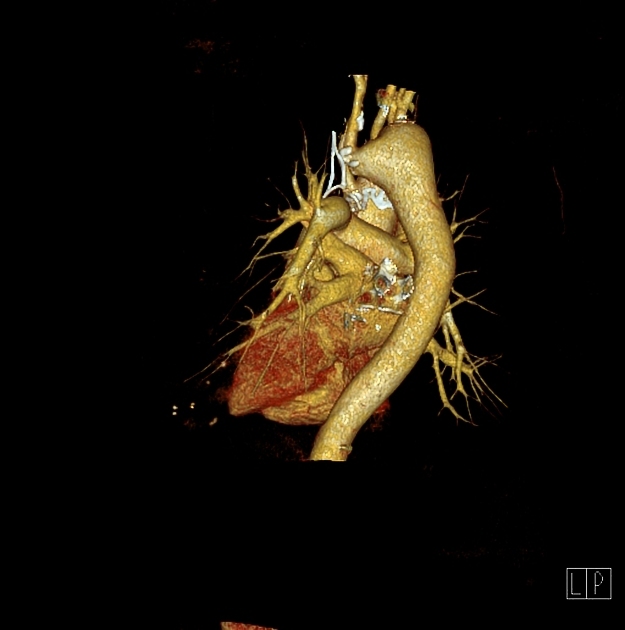
CT/MRI
Typically shows bulbous enlargement of the proximal subclavian artery at its origin from the aortic arch, posterior to the esophagus.
If the diameter of the bulbous diverticulum is 1.5 times greater at the base than in the distal subclavian artery then the ductus arteriosus / ligamentum arteriosum is located on the opposite side of the arch, forming a vascular ring. Conversely, if the subclavian artery is normal caliber at the base then the ductus / ligament is located on the same side as the arch and no vascular ring is present 8,11.
Treatment and prognosis
Given the rarity of this condition, there is no established management guideline. Options include aortic replacement or thoracic endovascular stent-graft replacement (TEVAR), and extra-anatomic bypass of the aberrant subclavian artery 6,7. Many consider surgical intervention once the diameter of the diverticulum orifice exceeds 30 mm, and/or the diameter of the descending aorta adjacent to the diverticulum exceeds 50 mm 8.
Complications
The major complications of Kommerell diverticulum are rupture or dissection 7.
History and etymology
It is named after Burckhard F Kommerell, a German radiologist (1901-1990) who first described it in 1936 8.









 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.