
Petersen hernias are internal hernias which occur in the potential space posterior to a gastrojejunostomy. This is herniation of intestinal loops through the defect between the small bowel limbs, the transverse mesocolon, and the retroperitoneum, after any type of gastrojejunostomy. The laparoscopic approach facilitates the occurrence of this type of hernia, due to the lack of post-operative adhesions which prevent bowel motility and hence, herniation.
On this page:
Epidemiology
The incidence of internal hernias following laparoscopic gastric bypass surgery ranges from 1.8-9.7%, much higher than that seen when this procedure is performed by open surgery 1.
Patients submitted in the past for surgical treatments for chronic peptic ulcer and its complications (antrectomy, truncal vagotomy, gastrojejunostomy, or subtotal gastrectomy in conjunction with gastrojejunostomy).
Clinical presentation
usually presents with diffuse abdominal pain (could be caused by bowel obstruction with spontaneous reduction)
-
may present as intestinal obstruction
late postoperative obstruction may be due to adhesions, fibrotic stenosis, intussusception or more often, internal hernias 1
Pathology
These hernias occur in patients with a Roux-en-Y gastric bypass:
-
this surgery is one of the preferred procedures for bariatric surgery
the minimum amount of the gastrointestinal tract that is excluded from intestinal transit is the distal stomach, part of the duodenum, and about 40 cm of the proximal jejunum
the gastric bypass may be done by open surgery or laparoscopy, the latter being preferred 1
-
the anastomotic loop may be retrocolic or antecolic
retrocolic anastomosis creates a space in the mesentery, opening the possibility of a transmesenteric hernia
Petersen hernia may occur in both types of anastomosis 1
Radiographic features
Investigative computed tomography scans and upper gastrointestinal and small bowel contrast studies may fail to reveal an internal hernia in 20% of cases 2.
CT
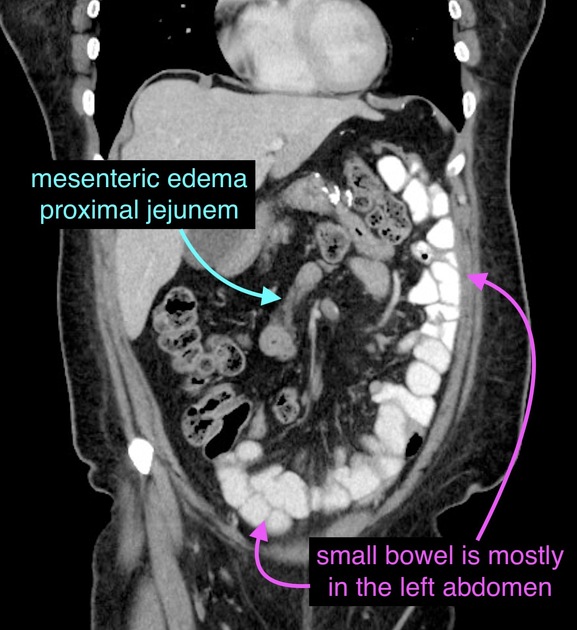
Signs of a Petersen hernia include:
upper abdominal distension 4
herniated intestinal loop segment above the gastric level
rotation of mesenteric vessels (whirl sign)
ligament of Treitz displaced anteriorly and to the right
middle-distal ileum courses downwards in the left hypochondrium 1
Treatment and prognosis
Treatment requires reduction of the incarcerated bowel and closure of the defect. Any nonviable bowel must be resected.
History and etymology
It was reported in 1900 by German surgeon Walther Petersen (1867-1922) 5, on the occurrence of an internal hernia after partial gastrectomy and gastrojejunostomy 3. The internet and the published literature are replete with misspellings of this eponym as 'Peterson'.






 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.