
Pseudocoarctation of the aorta is a rare anomaly characterized by elongation of the aortic arch associated with buckling at the level of the ligamentum arteriosum.
On this page:
Epidemiology
Associations
Reported associations include 3,9:
left cervical aortic arch
aortic aneurysm, dissection and rupture
Diagnosis
The CT appearance is characteristic, however, the definition depends on the catheter measurement of pressure gradient <20 mmHg ref. The absence of collateral arteries is important to distinguish pseudocoarctation from coarctation.
If the patient is asymptomatic with no evidence of complications, such as dissection or aneurysm, a CT diagnosis is sufficient.
Clinical presentation
An analysis of 18 cases from the literature could show bias towards symptomatic patients; the presentations were as follows9:
hypertension (55%), half with unequal upper limb blood pressure
dyspnea (17%)
back pain due to dissection (11%)
dysphagia (6%)
asymptomatic (11%j
Pathology
It is thought to be congenital, due to less than normal compression of the third to seventh dorsal aortic segments. The increased length accounts for the high position of the aortic arch and associated buckling.
Radiographic features
CT angiography
The following features are useful in diagnosis (according to case reports) 3:
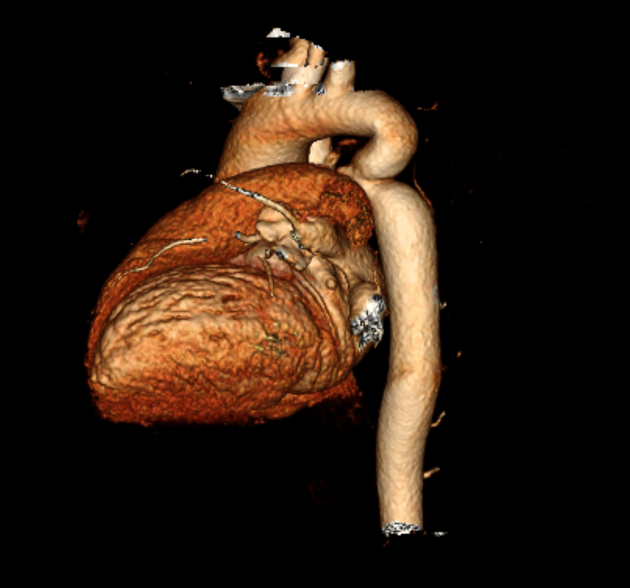
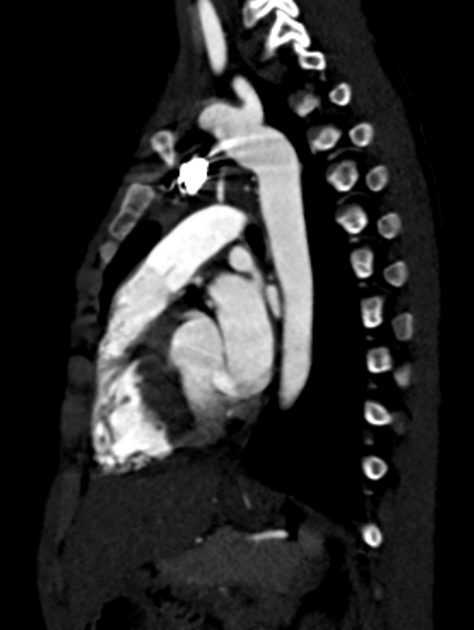
demonstration that the abnormal mass in the mediastinum is part of the aorta
unusually superior location of the top of the aortic arch
visualization of the isthmic portion of the descending thoracic aorta that's not adjacent to the spine, but rather ventral to it; this is surrounded by aerated lung
a more caudal origin of the subclavian artery
Other reported features include 2:
the aortic arch of pseudocoarctation is elongated and may arise higher than the clavicle (associated with cervical aortic arch)
absence or only a mild degree of stenosis of the aortic lumen
the absence of collateral circulation
the absence of left ventricular hypertrophy and ascending aortic dilation
Cardiac catheterization and angiography provide a definitive diagnosis.
Treatment and prognosis
It is considered a benign entity with no specific intervention 8. Some advocate surgical treatment for all symptomatic patients and those with associated aneurysm formation 7.
History and etymology
The first description of pseudocoarctation have been attributed to the Austrian Hugo Rösler and his American college Paul White in 1931 10,11. Later Dotter, Steinberg, Souders et al. described additional cases in 1951 3,5.
Differential diagnosis
Consider true coarctation of the aorta:
evidence of collateral circulation (e.g. rib notching)







 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.