
Presentation
Past history of a ruptured ovarian cyst. Severe right lower abdominal pain.
Patient Data
Age: 35 years
Gender: Female
Transabdominal US of the pelvis including the right iliac fossa was normal, therefore transvaginal imaging was performed.
From the case:
Acute appendicitis (transvaginal ultrasound)


Download
Info
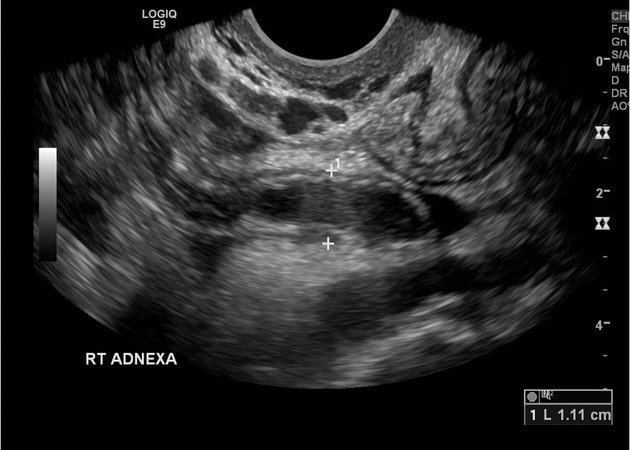
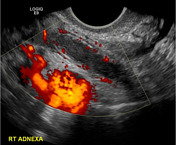
Right adnexal tender, fluid-filled, blind-ending tubular mass with surrounding free fluid. Increased blood flow in the wall of the tubular structure adjacent to iliac vessels.
Case Discussion
Despite this being a transvaginal examination, appearances are all consistent with acute appendicitis. Differential diagnosis is acute salpingitis but the tubular structure is blind-ending and not associated with the ovary.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.