
Presentation
Right lower quadrant pain and tenderness.
Patient Data
Age: 20 years
Gender: Male
From the case:
Acute appendicitis with CT arrowhead sign






Download
Info
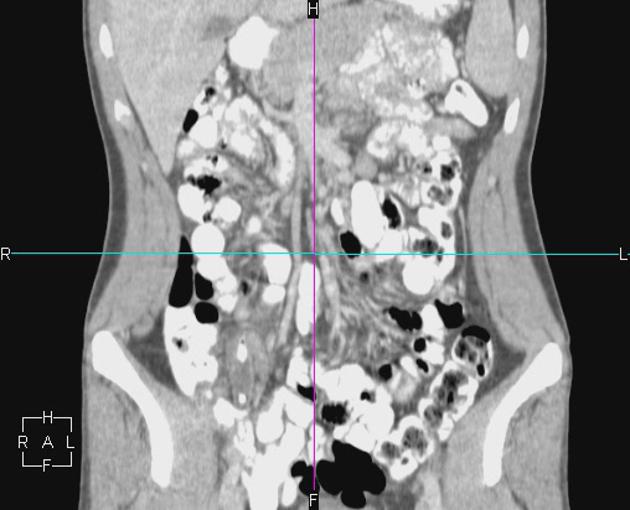
Dilatation of appendix and periappendiceal mesenteric fat stranding with an appendicolith in the appendiceal lumen. Mesenteric lymphadenopathy is distinguishable in the adjacent mesenteric fat.
Inflammation at the base of the appendix produces an 'arrow-like' collection of cecal contrast.
Local dilatation of the right ureter near the inflammation site is likely to represent a local response to the adjacent inflammation.
Case Discussion
Acute appendicitis is one of the commonest causes of an ‘‘acute abdomen’’ and appendectomy is the commonest emergency surgical operation performed worldwide. The two diagnostic CT signs of acute appendicitis are:
- unequivocal identification of an abnormal appendix: usually fluid-filled with a slightly thickened and circumferentially enhancing wall and dilated more than 6 mm in transverse diameter
- an appendicolith associated with pericaecal inflammatory stranding


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.