
Presentation
Car vs. pole at high speed. Hypotensive.
Patient Data


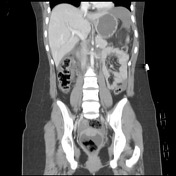
Extensive hepatic laceration is seen involving the inferior aspect of the right lobe of the liver extending to the level of the gallbladder fossa. This is associated with extensive perihepatic, hepatorenal high-density free fluid which tracks into the right paracolic gutter.
Right adrenal lesion, presumably traumatic hematoma.
Multiple splenic lacerations are demonstrated extending from the splenic cortex to the level of the splenic hilum with several foci of contrast extravasation consistent with active bleeding. A large amount of perisplenic hematoma is evident.
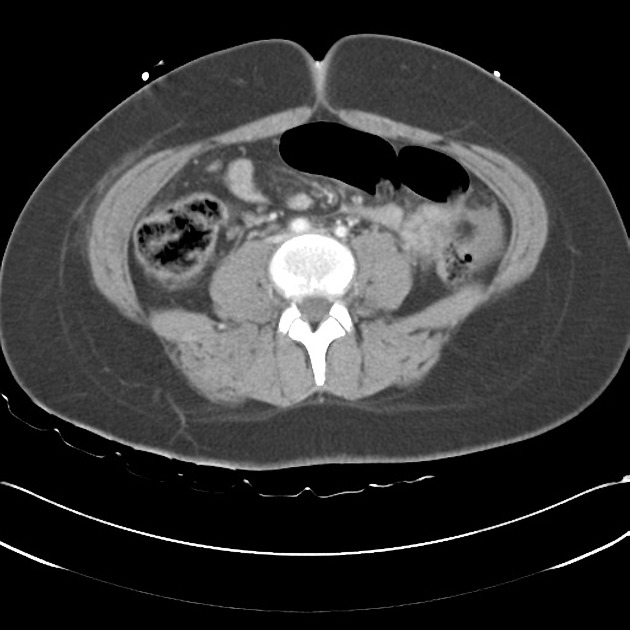
A linear defect is seen in the posterior wall of the third part of the duodenum which may suggest duodenal injury. The second and the third parts of the duodenum appear diffusely thickened, supporting that likelihood.
The uncinate process of the pancreas is suspiciously swollen and reduced in density, suggesting that both duodenum and pancreas are contused. Associated retroperitoneal fat stranding is seen.
Flattened IVC and small caliber abdominal aorta is consistent with the hypovolemic patient state.
The kidneys, adrenal glands appear to be intact.
Free fluid is seen within the pelvis presumably tracking inferiorly from the upper abdominal injuries, however no free intra-abdominal gas is identified.
Fractures of the tips of the right L1 to L4 transverse processes without further evidence of disruption of alignment or fractures of the lumbar spine.
Case Discussion
Injuries sustained:
- Extensive liver and splenic lacerations with evidence of active contrast extravasation from the splenic bed. Likely right adrenal hematoma.
- Possible duodenal and pancreatic injuries.
- L1-L4 right transverse process fractures.
Evidence of CT hypoperfusion complex (more commonly known as shock bowel) with flattened IVC and small caliber abdominal aorta.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.