
Presentation
History bladder tumor. Post surgery, BCG and interferon. PSA 5. Rule out prostate carcinoma.
Patient Data
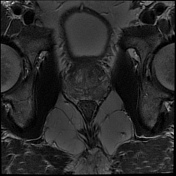

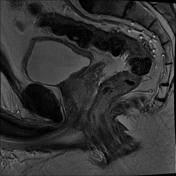
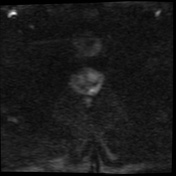
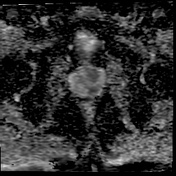
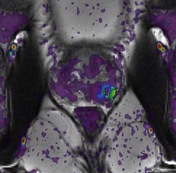
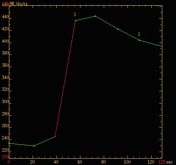

Focal highly suspicious lesion in the left posterior and posterolateral PZ base. Homogenous hypointense on T2WI. Broad-based capsular bulging raises the possibility of extracapsular invasion. Restricted diffusion with an ADC value of 550. Type 3 enhancement curve. Overall PIRADS score 5/5.
Case Discussion
TRUS biopsy showed granulomatous prostatitis and no carcinoma.
Granulomatous prostatitis is a well described known mimicker of prostate carcinoma, clinically and on MRI. Clinically it often presents with elevated PSA and a firm nodule on DRE. On MRI, the lesion demonstrates typical features of a highly suspicious neoplastic lesion.
Currently, histopathology is the only means of establishing the diagnosis and excluding a tumor.
Possible causes include previous intravesical BCG treatment for bladder carcinoma, TB prostatitis, previous intervention (eg TURP) and idiopathic.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.