Paravaginal myxoid liposarcoma
Updates to Case Attributes
At gynecological examination: nodular neoformation hard - smooth, posterior in the fornix. Speculum: epithelial portions: dystrophies, no atypical vaginal dichargesdischarge. Eco office TV
TV ultrasound: hysterometry mm 75 x 36 regular morphology, linear endocavitary echoes mm 3.7, Rounded hypoechoic mass with net margin of 25 mm in diameter at the back of the cervix (myoma of the ligament?) non-liquid swelling free endopelvic. No ovarian abnormalities.
INIn the MRI report weit was suggested to remove the mass becousebecause there were signs that could be referred towere concerning for malignancy.
Histological findings: The neoformation is characterized by the proliferation of elements sometimes fused in a pattern mixo-fibrosarcoma-like at the most distinct pleomorphic plurinucleates with MFH-like aspects. They are observed numerous lipoblasts often pleomorphic immersed in a mixoid stroma rich in capillary vessels. The mitotic index is high (> 3-4 myths xhpf), no necrosis sites are observed and the neoplasia reaches the margins of surgical exeresisexcision. To immunocytochemistry proliferating elements express positive for CdK4 (clone EPR4513-32-7), CD 34 (clone QBEnd / 10), MDM2 (clone IF2), S-100 (polyclonal) and Vimentina (clone V9) while negative for 1-A-2-N- EMA (clone E29), desmin (clone DE-R-11), cytokerite (clone AE1-AE3) and smooth muscle alpha-actin (clone 1A4). KI67 (clone 30-9) is expressed in 20% of proliferating elements.
-<p>At gynecological examination: nodular neoformation hard - smooth, posterior in the fornix. Speculum: epithelial portions: dystrophies, no atypical vaginal dicharges. Eco office TV: hysterometry mm 75 x 36 regular morphology, linear endocavitary echoes mm 3.7, Rounded hypoechoic mass with net margin of 25 mm in diameter at the back of the cervix (myoma of the ligament? ) non-liquid swelling free endopelvic. No ovarian abnormalities.</p><p>IN MRI report we suggested to remove the mass becouse there were signs that could be referred to malignancy.</p><p>Histological findings: The neoformation is characterized by the proliferation of elements sometimes fused in a pattern mixo-fibrosarcoma-like at the most distinct pleomorphic plurinucleates with MFH-like aspects. They are observed numerous lipoblasts often pleomorphic immersed in a mixoid stroma rich in capillary vessels. The mitotic index is high (> 3-4 myths xhpf), no necrosis sites are observed and the neoplasia reaches the margins of surgical exeresis. To immunocytochemistry proliferating elements express positive for CdK4 (clone EPR4513-32-7), CD 34 (clone QBEnd / 10), MDM2 (clone IF2), S-100 (polyclonal) and Vimentina (clone V9) while negative for 1-A-2-N- EMA (clone E29), desmin (clone DE-R-11), cytokerite (clone AE1-AE3) and smooth muscle alpha-actin (clone 1A4). KI67 (clone 30-9) is expressed in 20% of proliferating elements.</p><p> </p>- +<p>At gynecological examination: nodular neoformation hard - smooth, posterior in the fornix. Speculum: epithelial portions: dystrophies, no atypical vaginal discharge. </p><p>TV ultrasound: Rounded hypoechoic mass with net margin of 25 mm in diameter at the back of the cervix (myoma of the ligament?) non-liquid swelling free endopelvic. No ovarian abnormalities.</p><p>In the MRI report it was suggested to remove the mass because there were signs that were concerning for malignancy. </p><p>Histological findings: The neoformation is characterized by the proliferation of elements sometimes fused in a pattern mixo-fibrosarcoma-like at the most distinct pleomorphic plurinucleates with MFH-like aspects. They are observed numerous lipoblasts often pleomorphic immersed in a mixoid stroma rich in capillary vessels. The mitotic index is high (> 3-4 myths xhpf), no necrosis sites are observed and the neoplasia reaches the margins of surgical excision. To immunocytochemistry proliferating elements express positive for CdK4 (clone EPR4513-32-7), CD 34 (clone QBEnd / 10), MDM2 (clone IF2), S-100 (polyclonal) and Vimentina (clone V9) while negative for 1-A-2-N- EMA (clone E29), desmin (clone DE-R-11), cytokerite (clone AE1-AE3) and smooth muscle alpha-actin (clone 1A4). KI67 (clone 30-9) is expressed in 20% of proliferating elements.</p>
Systems changed:
- Oncology
Updates to Study Attributes
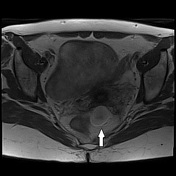
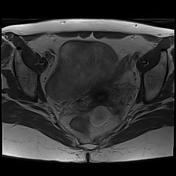
ovalOval mass, with greater axis of three centimeters, posterior to the vagina, that in the lower side comes close to the left wall of the rectum.
The mass has smooth margins, homogeneous low signal in T1 and appears hyperintense in T2 even in seq Fat Sat,on the fat sat sequence (fluid appearance - does not contain hemoglobin degradation products), and with homogeneous signal intensification after administration of gadolinium chelate. It exhibits hyperintensity of signal in the diffusion-weighed sequences, without any aspect of diffusivity restriction in the ADC map.
Image MRI (T2) ( update )

Image MRI (T2 fat sat) ( update )

Image MRI (T2) ( update )

Image MRI (T2) ( update )
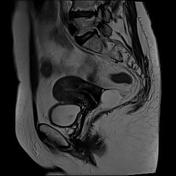
Image MRI (DWI) ( update )

Image MRI (ADC) ( update )

Image MRI (T1) ( update )
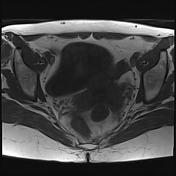
Image MRI (T1 C+) ( update )
Updates to Study Attributes
ovalOval mass, with greater axis of three centimeters, posterior to the vagina, that in the lower side comes close to the left wall of the rectum.
The mass has smooth margins, homogeneous low signal in T1 and appears hyperintense in T2 even in seq Fat Sat,on the fat sat sequence (fluid appearance - does not contain hemoglobin degradation products), and with homogeneous signal intensification after administration of gadolinium chelate. It exhibits hyperintensity of signal in the diffusion-weighed sequences, without any aspect of diffusivity restriction in the ADC map.
Image Annotated image (Axial T2) ( update )

Image Annotated image (Coronal T2) ( update )
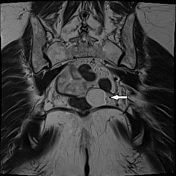
Image Annotated image (Sagittal T2) ( update )

Image Annotated image (Axial T1) ( update )

Image Annotated image (Axial T1 C+) ( update )