
Presentation
6 weeks of increasing abdo pain and unintentional weight loss. Tender RUQ. Deranged LFTs. Lives in SE Asia 6 months a year.
Patient Data



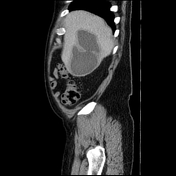
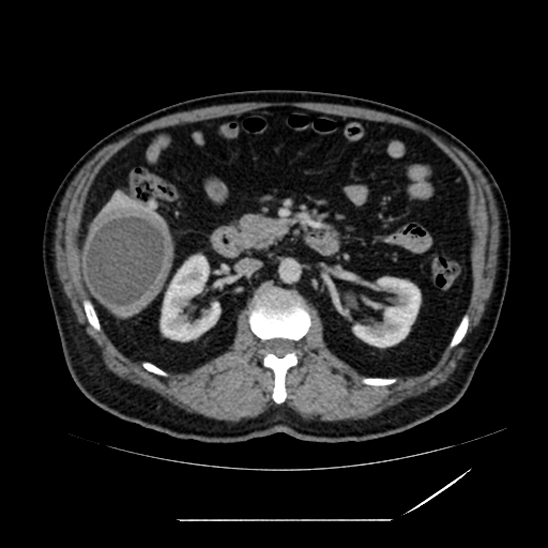
Right hepatic loculated cystic lesion with thick walls approx 7 x 7 cm axially and 12 cm caudocranially. No wall enhancement. No vascular involvement. No septae or calcified internal cyst contents. Small subcapsular cyst in segment IVa/VIII.
DDx amoebic abscess, hydatid disease or cystic malignancy. Drainage is recommended under US guidance.


Procedural sedation.
Ultrasound-guided 18-gauge entry needle into the right liver collection through a small amount of normal liver. Location within collection confirmed with contrast. A 12 French Dawson-Mueller locking pigtail catheter was placed over an Amplatz wire under fluoroscopy.
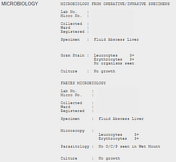
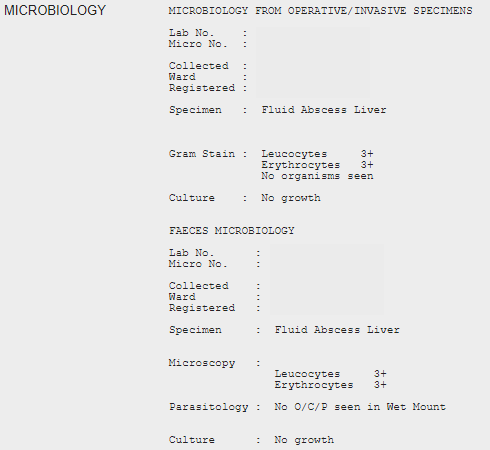
Approximately 300 ml of thick brown purulent fluid was aspirated and the sample was sent for pathology.
Drain secured with skin sutures.


Interval drainage of the right liver abscess. The drainage catheter has been removed. Two tiny residual subcapsular fluid foci remain with a total volume of <2cc. Hypoattenuation of the surrounding parenchyma reflects resolving inflammatory change. A tiny volume of low-density fluid along the capsular surface at the drainage site with mild adjacent fat stranding is considered within expected limitations. Otherwise, there is no intra-abdominal free fluid. No evidence of haemorrhage into the collections or peritoneal space. No new collection demonstrated. The small subcapsular cyst in segment IVa/VIII is unchanged from prior imaging.
Case Discussion
In addition to drainage, the patient was treated with oral metronidazole and paromomycin and recovered well.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.