
Presentation
Left upper limb weakness and partial seizure.
Patient Data









Large extra-axial mass, both solid and cystic, with homogeneous enhancement, localised in the right posterior frontal region with a large dural attachment and adjacent skull erosion. There is local mass effect.










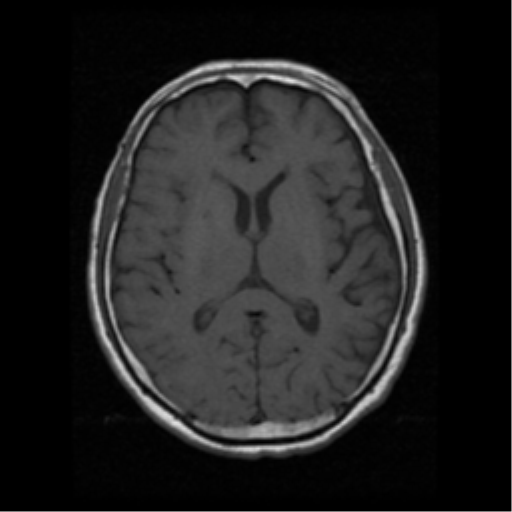
Large well-defined extra-axial mass in the right posterior frontal region with a large dural attachment and adjacent skull erosion. It appears durally based. The lesion measures 50 x 44 x 42 mm (AP by transverse by CC). It is both solid and cystic, with a large solid component anterolaterally and complex septated cystic component posteromedially and inferiorly. The solid component is mildly T2 and FLAIR hyperintense, with marked restricted diffusion and mild to moderate reasonably uniform enhancement. No flow voids seen. The wall of the lesion is enhancing, with minor irregularity. The septa of the cystic portion also enhancing. Posteromedially, there is a mild degree of vasogenic oedema. Local mass-effect is present causing only 2 mm midline shift without ventricular effacement or obstruction. MR perfusion shows increase in CBV (not shown). Spectroscopy trace adds little (not shown). At the osseous component, the margin of destruction is clear with no surrounding enhancement for hyperostosis on CT.
No other intra or extra-axial lesion identified. The remainder of the study is unremarkable.

The patient underwent to a surgical resection.
MICROSCOPIC DESCRIPTION:
The sections show a meningioma with increased cellularity. The tumour forms solid sheets as well as scattered whorls. The tumour cells have enlarged and mildly pleomorphic nuclei with focal prominent nucleoli. There are up to 16 mitoses per 10 high power fields. Areas of necrosis are seen. Cerebral cortex is present and there is no evidence of brain invasion. The tumour invades through the dura into the skull bone. It involves the entire thickness of the bone through the cortex and it is 0.1mm from the outer periosteum. The tumour involves the circumferential radial bony margin. There is no evidence of malignant change. The features are those of atypical meningioma. The Ki-67 index is about 20%. About 10% of the tumour cells are weakly progesterone receptor positive.
DIAGNOSIS:
Atypical meningioma with full thickness invasion into skull bone (WHO Grade II).
Case Discussion
CT and MRI studies show a large complex extra-axial mass right posterior frontal region with bone involvement. Differential diagnosis includes dural metastasis, meningioma and haemangipericytoma.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.