
Presentation
This young man presented with an altered conscious level. The initial concern was of neurological infection.
Patient Data
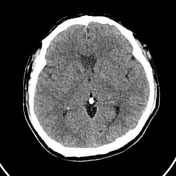


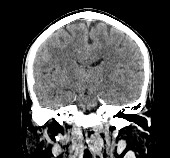

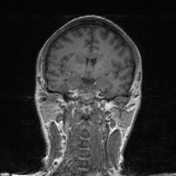
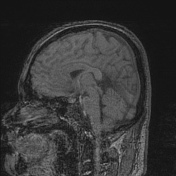
Low attenuation in the rostrum and genu of the corpus callosum.
Ill-defined hypoattenuation foci in the anterior limb of the internal capsule, centrum semiovale and mesial temporal lobe on the right.
No hemorrhage.
The remainder of the intracranial appearances is normal.
Comment: The appearances are those of acute infarction, the distribution of the infarction and involvement of the corpus callosum is unusual. This suggests both ACA and MCA peforator involvement.
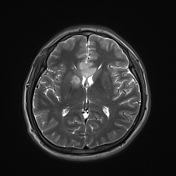
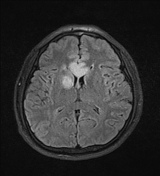
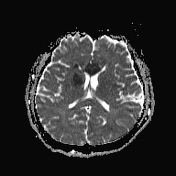
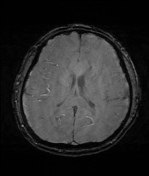
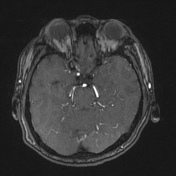
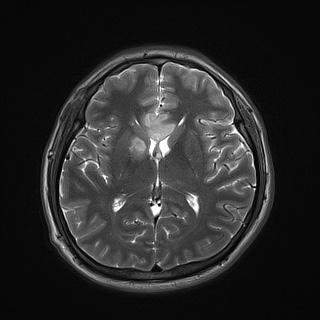
Extensive restricted diffusion in the rostrum, genu and body of the corpus callosum. Further foci of restricted diffusion of variable size in the right internal capsule, corpus striatum, centrum semiovale and insula. All consistent with acute infarcts.
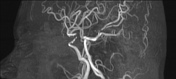
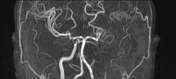
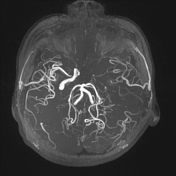
The left ICA lumen is severely narrowed and occluded from its cavernous portion, with a minimal flow signal in the left MCA.
On the right, there is a high-grade stenosis of the supraclinoid ICA (C6/7 segments).
No signal flow identified within the anterior communicating and anterior cerebral arteries.
Comment:
1. Appearances are those of multifocal ACA and right MCA territory acute infarction.
2. Left ICA severe narrowing with occlusion from its cavernous segment. Right supraclinoid ICA high-grade stenosis. No signs of flow signal within the anterior cerebral arteries.
Given this patient is categorized as a 'Young Stroke' and unusual infarct distribution further workup should be considered, in particular a cardioembolic source or vasculitis should be sought. "
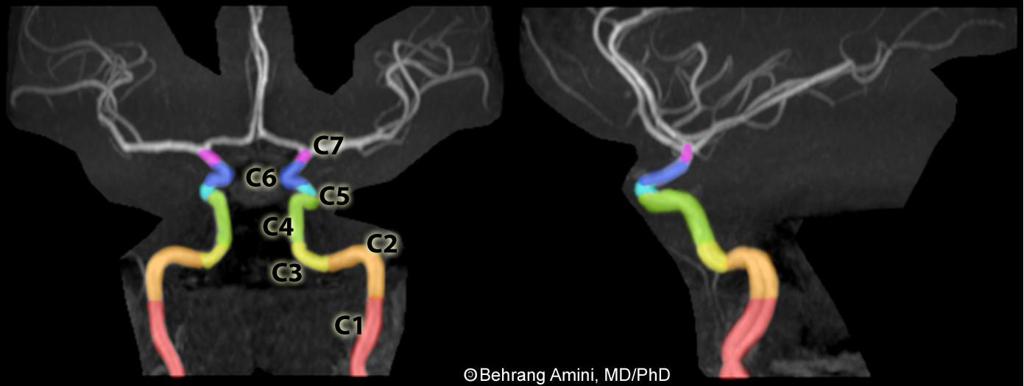
From case https://radiopaedia.org/cases/carotid-artery-segments-diagram
Case Discussion
One of the more unusual distributions of infarction at presentation, with the admission CT indicating corpus callosal involvement indicative of an anterior cerebral artery territory stroke.
It also implies middle cerebral artery involvement making this dual territory.
Furthermore the young age of the patient and initially atypical symptomatology suggests this is not a straightforward cause.
A subsequent vegetation on the aortic valve was identifed at echocardiography in keeping with bacterial endocarditis.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.