
Presentation
History of transient ischemic attacks (TIA)
Patient Data

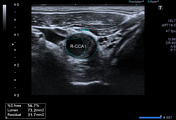
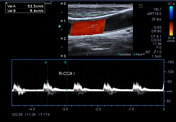
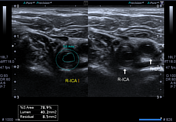





Intima-media thickness is increased diffusely with variable thickness predominantly hypoechoic plaques (type-1) causing 78% of area stenosis in the right proximal ICA. However, no significant difference in Peak systolic velocity of CCA and ICA is noted (53cm/sec vs 77cm/sec). Also, there is no color aliasing at the site of maximum stenosis in right ICA.

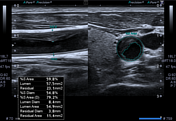
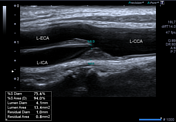

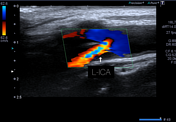



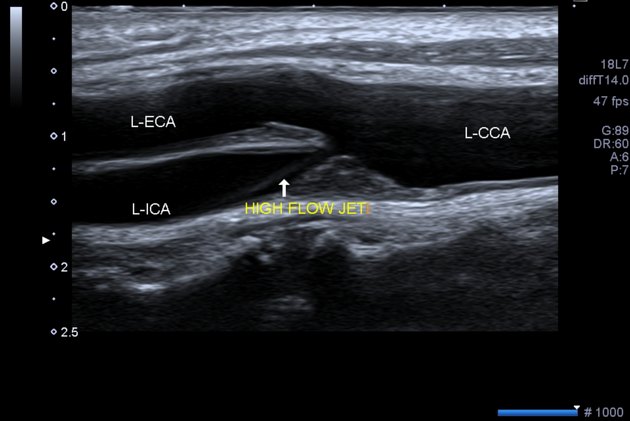
A hypoechoic (type-1) smooth surfaced plaque is noted in left carotid bifurcation and carotid bulb causing 75.6% of diameter reduction of left proximal ICA on greyscale. An echogenic high flow jet is also visible on greyscale arising from the site of stenosis. Color Aliasing is appreciable with high PRF (high color scale) at the level of the carotid bulb.
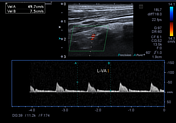
Spectral Doppler analysis shows a high Peak systolic velocity (PSV) of 256cm/sec and an End-diastolic velocity of 98cm/sec in ICA as compared to a PSV of 60cm/sec in ipsilateral CCA with ICA/CCA PSV ratio of more than 4.
Case Discussion
Above mentioned findings are in keeping with more than 70% stenosis of left ICA but less than near occlusion as per the Society of Radiologists in Ultrasound (SRU) consensus guidelines.
As per the Sonographic NASCET Index, there is 70-79% stenosis in the left ICA.
No internalization of flow is noted in bilateral external carotids.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.