
Presentation
Hypovolaemic shock.
Patient Data



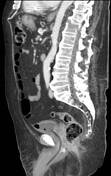
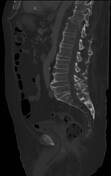
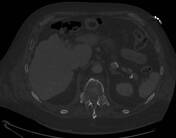

Horizontal fracture through T12 body below the superior endplate, right pars interarticularis, and spinous process; involves both costovertebral joints and extends as nondisplaced fracture in head of left 12th rib. The fracture also involves the anterolateral part of the T11-T12 syndesmophyte on both sides.
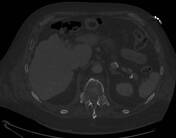
Large, partially thrombosed, subcutaneous haematoma in right hip, measuring 8.7 x 6.9 x 16.2 cm.
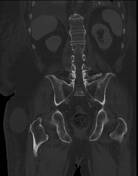
Syndesmophytes; ossification of the supraspinous ligament, ossified iliolumbar ligaments, and partially fused sacroiliac joints - taken together, these findings are highly suggestive of ankylosing spondylitis.
Tip of NGT barely passes the gastrooesophageal junction.
Bilateral pleural effusion.
Minimal pneumobilia in left hepatic lobe, probably due to ERCP.
Calcified pedunculated aneurysm measuring 15 x 11 mm from bifurcation of coeliac trunk into common hepatic artery and splenic artery (left gastric artery originates proximally to the bifurcation). Calcified saccular aneurysm measuring 21 x 16 mm in the middle of the splenic artery.
Tiny cyst in pancreatic neck.
Few tiny cortical cysts in both kidneys.
Leads from dual-chamber pacemaker at upper edge of scan.
Case Discussion
Presented to the ED with hypovolaemic shock, on NOAC therapy - CT/CTA abdomen-pelvis ordered due to suspected retroperitoneal or gastrointestinal haemorrhage. Signs of ankylosing spondylitis, a chalk stick fracture though the T12 vertebra, and a large pelvic subcutaneous haematoma were discovered at CT. Further questioning of the live-in caretaker revealed that the patient had fallen at home 10 days earlier.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.