
Presentation
A nonsmoking, man with no previous comorbidities, attended to us for painless inflammation and oedema of left ankle and foot for at least 7 months, without fever or other joint swellings. There was no history of trauma. He was seen in the emergency department 2 months ago, he was diagnosed with cellulitis and oral antibiotics were prescribed. Physical examination revealed oedematous, hyperaemic leg and foot, with absent arch (mid-foot collapse), hyperpigmentation, and calluses at pressure points. HbA1c laboratory tests = 14, 9%. He had undiagnosed diabetes.
Patient Data



Weight-bearing dorsoplantar and lateral foot radiographs:
lateral dislocation of the 2nd to 5th tarsometatarsal joints.
bony fragmentation and collapse of the Midfoot with rocker-bottom deformity.
severe tarsal bones arthropathy and joint destruction.
diffuse bony sclerosis and remodelling
increased soft tissue thickness around the foot and ankle.
All these findings are consistent with chronic Charcot's joint (neuropathic arthropathy).


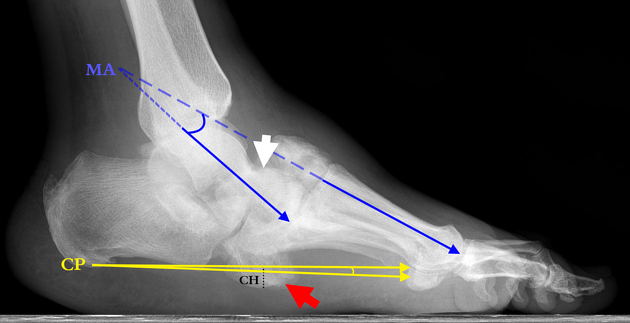
Weight-bearing lateral view:
White arrow: Inferior luxation of the talar head
Red Arrow: cuboid - becoming the most inferior bone of the foot
MA: Talar- First metatarsal angle (Increase of the Meary angle) = 18.2°
CP: Calcaneal pitch angle (Decrease of the calcaneal pitch) = 1.4°
CH: cuboid height = Negative (-1.6 mm)
Weight-bearing frontal view:
White arrow: There is an increased joint space between metatarsal bone I and II indicating Lisfranc's joint dislocation with lateral displacement of the metatarsal bones.
Dotted: shows disorganised tarsometatarsal joints and osteopenia and cartilage fragmentation
Navicular (Yellow) and medial cuneiform (Red) are dislocated (The navicular cuneiform joint is dislocated medially)
Blue arrow: Erosion of the lateral surface of the lateral cuneiform and 5th metatarsal base
Case Discussion
Charcot neuroarthropathy is a progressive, noninfectious, destructive inflammatory process of joints associated with a deficit of pain sensation and proprioception. At the foot and the ankle, diabetes and polyneuropathy are the most frequent causes 1. It can lead to severe deformities and increased risk of amputation and death 2.
In the majority of diabetes-induced Charcot Foot, the initial diagnosis is delayed, especially in developing countries 3. This is due to poor knowledge of this rare condition by physicians 4. Early diagnosis and elimination of weight bearing will reduce articular destruction and major deformity.
On the other hand, it can reveal undiagnosed diabetes, as in this case. That is why any patient with a Lisfranc fracture, dislocation or foot deformity without trauma, should undergo evaluation for diabetes and other causes of sensory neuropathy 5.
Conventional radiography (especially lateral weight-bearing incidence) is generally the main imaging modality to diagnose, stage, and monitor the Charcot foot 6,7.
The radiographic features of a Charcot joint can be remembered by using the following mnemonics: 6 D8.
dense bones (subchondral sclerosis)
degeneration
destruction of articular cartilage
deformity (pencil-point deformity of metatarsal heads)
debris (loose bodies)
dislocation
Radiographic measurements: Three typical measurements help to determine the degree of the deformation 9:
Meary's angle (MA): also known as the Talar- First metatarsal angle. The angle between the long axis of the talus and the long axis of the first metatarsal. Normal value should be around 0°.
Calcaneal Pitch angle (CP): Angle between the inferior margin of the calcaneus and a line from the inferior weight bearing point of the calcaneus and the base of the fifth metatarsal. Normal value lies between 20 and 30°.
Cuboid height (CH): Perpendicular distance from the plantar aspect of the cuboid to a line drawn from the plantar surface of the calcaneal tuberosity to the plantar aspect of the fifth metatarsal head. Mean normal value is about 1.2 cm above that line.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.