
Presentation
Chronic headaches, bilateral upper limb weakness and paraesthesia, and persistent vertigo.
Patient Data
















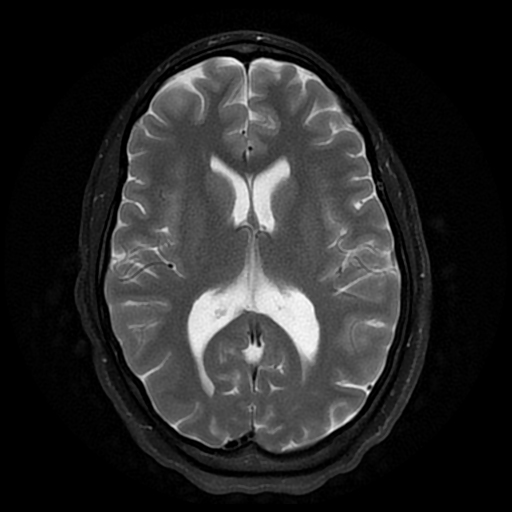
There is a cerebellar tonsillar herniation of approximately 10.4 mm and associated herniation of the medulla oblongata. There is associated hydrosyringomyelia of the cervical cord. Contrast-enhanced MRI brain is otherwise normal.










MRI Mobitrak confirms an extensive hydrosyringomyelia extending from the craniocervical junction to the T10 level approximately.
Case Discussion
Features consistent with Chiari 1.5 malformation with a cerebellar tonsillar and medulla oblongata herniation and expected crowded posterior fossa. Chiari 1.5 malformation is often diagnosed with an inferior cerebellar descend or herniation of approximately 12mm or more. In this instance, the herniation measured approximately 10.4 mm however there is a well-identified medulla oblongata herniation, suggesting the progression of a type 1 Chiari malformation. There is an associated severe hydrosyringomyelia from the base of the skull to the T10 vertebral level. There is no hydrocephalus, a normal odontoid process, and no scoliosis.
Case courtesy of Dr K Kobo and Dr IA Nagdee.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.