
Presentation
History of colonic mass resection, recurrent chest infection. Chest tube placement for recurrent effusion, chest tube oozing stool.
Patient Data




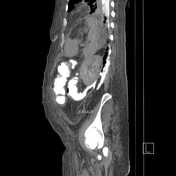



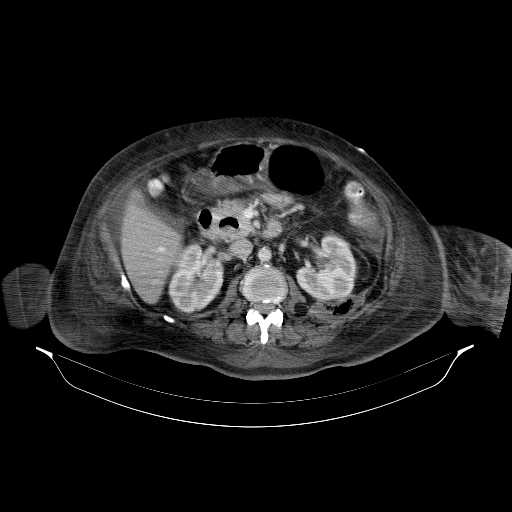
The prominent finding on this study is a defect in the posterior wall of the middle part of the descending colon with tracking of contrast through the left retroperitoneum.
After instilling contrast via rectal enema, it leaks through the defect in the inferior aspect of the posteromedial left parietal pleura to collect in the left costophrenic recess of the pleural cavity.
Case Discussion
The key to this diagnosis is to follow the course of the contrast material which, after having been injected through the rectum, crosses into the pleural cavity. That, coupled with relevant clinical history and the chest tube oozing stool cinch the diagnosis of a colopleural fistula.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.