
Presentation
Jaundice, right hypochondrial pain, nausea and fever. Known HIV positive.
Patient Data



Abdominal X-rays confirm the absence of calcific cholelithiasis. There is a right basal pleural effusion.
There is a non-specific bowel gas pattern with evidence of abdominal pain. X-rays are otherwise unremarkable. There is a previous sterilisation.

Upper abdominal ultrasound demonstrates :
hepatic steatosis
cholelithiasis, no cholecystitis
intrahepatic and extrahepatic bile duct distention
normal pancreas and pancreatic duct
necrotic mesenteric, para-aortic and porta-hepatic lymph nodes (HIV positive)
Cine loops of the ultrasound demonstrate intra and extrahepatic bile duct distention, with echogenic calculi causing posterior acoustic shadowing within the intrahepatic bile ducts, common hepatic and common bile ducts.
There is necrotic porta hepatic lymph adenopathy in keeping with the positive HIV status and possible abdominal tuberculosis/ tuberculous lymph adenitis.








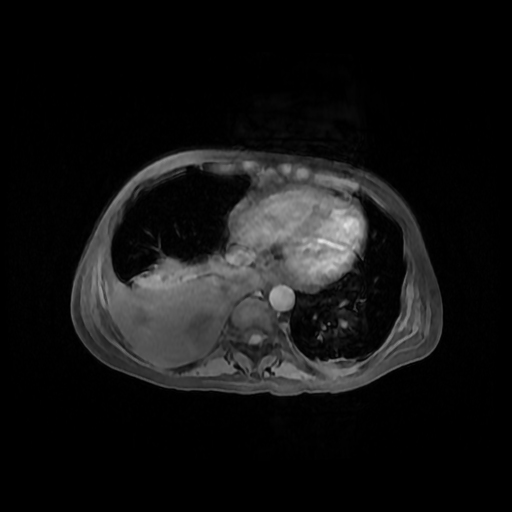
There is a large, right pleural effusion (10 HU), with compressive atelectasis. There is a tiny left basal effusion. There are no other thoracic abnormalities to suggest pulmonary tuberculosis.
There is hepatic steatosis, with dilated intra and extrahepatic bile ducts with a collapsed distal common bile duct (CBD). There are ill-defined punctate densities within the dilated ducts. There is no hepatomegaly.
The gallbladder is contracted with punctate calcified gallstones. There is no cholecystitis.
The pancreas and pancreatic duct are normal.
There is an isolated spenic cyst, with a normal splenic size.
There is necrotic epigastric, portahepatic, paraaortic and paracaval lymphadenopathy.
Suspected intestinal/ abdominal tuberculosis with abnormal small and large bowel including the terminal ileum.
Complex pelvic appearance suggesting pelvic sepsis (tubo-ovarian complexes/pelvic inflammatory disease/possible urogenital tuberculosis).












MRI of the upper abdomen and MRCP confirm dilated intrahepatic bile ducts with hepatolithiasis. Ductal enhancement suggests associated cholangitis.
There is a proximal common bile duct stricture. There is upstream choledocholithiasis with calculi within the common hepatic bile duct and proximal common bile duct. This is well demonstrated in the coronal sequences and reformats.
There is cholelithiasis and no cholecystitis.
The pancreas and pancreatic duct are normal.
There is a large right pleural effusion, a tiny left pleural effusion and minimal perihepatic fluid. There extra skeletal soft tissue oedema.
Image courtesy: Dr IA Nagdee
Case Discussion
An example of a partial, tight, proximal CBD stricture with upstream biliary stasis and consequent development of cholelithiasis, hepatolithiasis and choledocholithiasis. She was referred to the hepato-biliary team for further management. ERCP confirmed the bile duct stricture. With the performance of a sphincterotomy, and stricture dilatation, there has been significant drainage of the calculi and obstructed bile. An elective cholecystectomy is planned.
There is a complicated background clinical history of immune suppression (HIV positive), large right pleural effusion requiring drainage, suspected abdominal/ intestinal tuberculosis and tuberculous lymphadenitis, and possible urogenital tuberculosis/pelvic inflammatory disease.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.