
Presentation
A heavy smoker with a past medical history of asthma-COPD overlap syndrome, presented with dyspnea and chest pain.
Patient Data




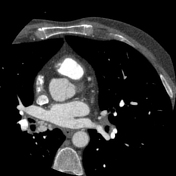



The left main stem coronary artery shows a small calcified atheromatous plaque not causing significant stenosis.
Multiple calcified atheromatous plaques were seen in the LAD artery, causing up to 50% stenosis in the proximal part.
The left circumflex artery shows a small calcified atheromatous plaque causing mild narrowing.
There is marked enlargement and tortuosity of the right bronchial artery, with communication with one of the branches of the circumflex artery near the right hilum. Features are suggestive of a coronary artery fistula between branches of the left circumflex artery and the right bronchial artery.
Lung images show bilateral emphysematous changes.
Case Discussion
The patient underwent cardiac catheterization, which revealed a fistula involving one of the left circumflex artery distal segments, most likely to the right bronchial arterial branches, reinforcing previous imaging results.
A coronary-bronchial artery fistula is an abnormal connection between a coronary artery and a bronchial artery (left circumflex branches and right bronchial arteries in our case), potentially leading to blood flow diversion away from the heart's circulation, posing risks like myocardial ischemia or heart failure.
Treatment often involves embolization or surgical intervention to correct the abnormal connection.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.