
Presentation
Known Crohn's disease presenting for MR enterography. Incidental finding.
Patient Data


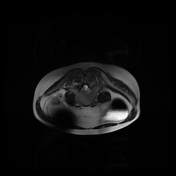
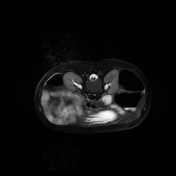
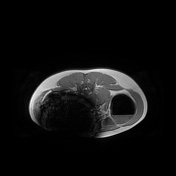
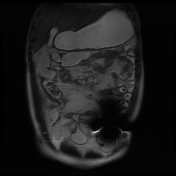

Bowel distortion with strictures, and fistulae identified within the right iliac fossa involving the terminal ileum. Specifically, the identification of multiple ileo-ileal and ileocolonic ( ascending and sigmoid colon) fistulae. There were no abscesses or collections.
MRI enterography was prematurely curtailed and halted once a central pelvic and left iliac fossa metallic artifact was realized.

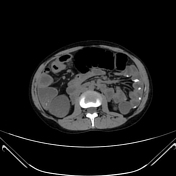




Due to the metallic artifact, the requested MRI enterography was converted to a CT study.
CT scanogram demonstrates a metallic density within the right hemiabdomen, specifically a trapped capsule endoscope. This was confirmed to be intraluminal, within an ileal loop.
Scattered barium is identified throughout the fluid-filled gastrointestinal tract due to the oral administration of dilute barium and Osmitrol solution for the MRI enterography study.
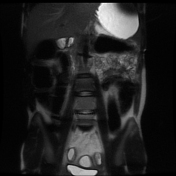
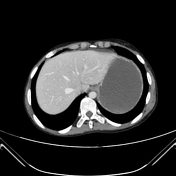
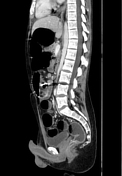
There is hyperenhancement and thickened small bowel loops in the right hemiabdomen and recto-sigmoid colon. There are strictures of the terminal ileum and multiple entero-enteric and entero-colonic fistulae within the right iliac fossa. There is variable prestenotic dilatation of the ileum and recto-sigmoid colon.
There are no abscesses or drainable collections. The hepato-biliary tract, renal tract, pancreas and sacroiliac joints are normal with no extraintestinal complications of Crohn's disease.
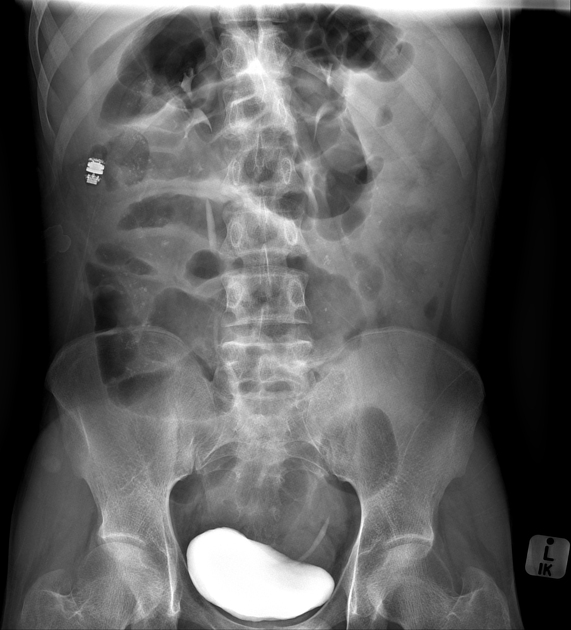
The abdominal X-ray was performed post the MRI and CT study and confirmed the trapped capsule endoscope within the right hypochondrium. There is an eccentric bowel gas pattern concordant with CT findings. The punctate radiodensities represent dilute barium. Opacified renal tract post-CT intravenous contrast administration.
Case Discussion
The history of previous capsule endoscopy and possible trapped capsule endoscope was not conveyed prior to the request and performance of MRI enterography. There was no prior request for imaging to identify a trapped endoscope or even a patency capsule on record. Once the metallic artifact was identified, the MRI study was halted. Capsule endoscopes are not MRI compatible, hence MRI studies are contraindicated in these instances. Fortunately, in this instance, no complications occurred. This incident triggered a more detailed screening for MRI enterography patients and consideration for an abdominal X-ray prior to study in suspicious circumstances. The metallic artifact appeared within the central pelvis and left iliac fossa, and amazingly the trapped capsule endoscope was found to be intraluminal, right-sided and possibly moved during the MRI performance.
The study confirmed complicated Crohn's disease by the presence of mid to distal ileal, distortion, pre-stenotic dilatation and multiple entero-enteric and entero-colonic fistulae and strictures.
Case courtesy: Dr M.N.Patel


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.