
Presentation
Fibroid uterus, status post 3 cesarean sections. Omental and peritoneal fibroids encountered during last C-section. MRI done 2 months later.
Patient Data

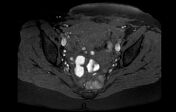
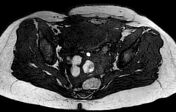
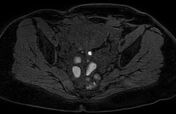

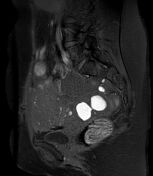

Postoperative changes status post C-section. Fullness measuring 6.2 x 2.1 x 5.3 cm in the plane between the uterus and the urinary bladder, showing heterogeneous signal, including artifacts from surgical staples and/or hemostatic material, small hematoma/blood products, and oval structures. Said oval structures at the right aspect of the fullness at the anterior aspect of the pelvis, show early peripheral enhancement, then progressive enhancement. Adhesions between the lower uterine segment and the urinary bladder.
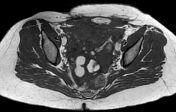
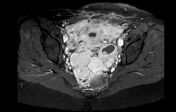
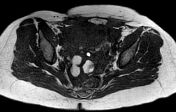
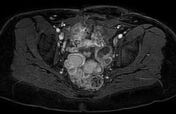
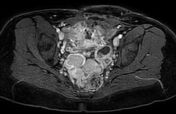
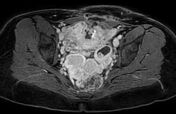
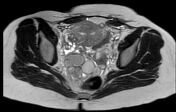
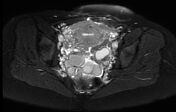
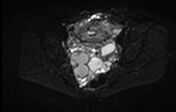
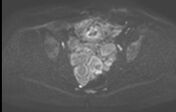
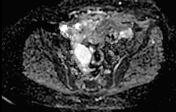
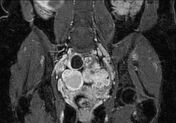
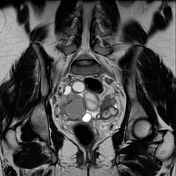
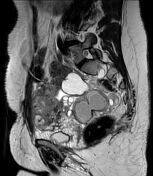
Numerous lesions in the rectouterine pouch, forming the semblance of a large mass; some are multilobular and some contain blood products. On both sides of the pelvis are complex cystic structures with a solid component; on the right, up to 4.7 cm in the long axis, with peripheral enhancement and on the left, 3.1 cm with an internal solid component. No clear separation plane between the oval structures in the rectouterine pouch and the rectal wall.
Small soft tissue foci pepper the peritoneum, for example: in the right pelvis, superior to the inguinal canal, and in the abdominal wall, for example: at the level of the surgical incision on the left.
Anteverted and anteflexed septate uterus. Endometrial thickness - 0.5 cm. Junctional zone not well-defined. The ovaries are normal in size and position.
Conclusion:
Taking into account the clinical and pathologic findings (see Discussion), the radiographic findings are compatible with disseminated peritoneal leiomyomatosis, although several foci are suggestive of deep pelvic endometriosis.



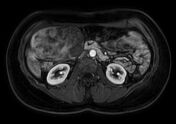





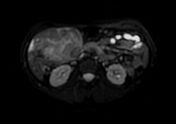



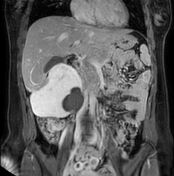
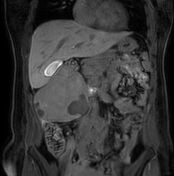



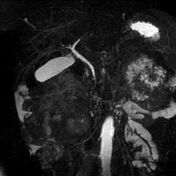
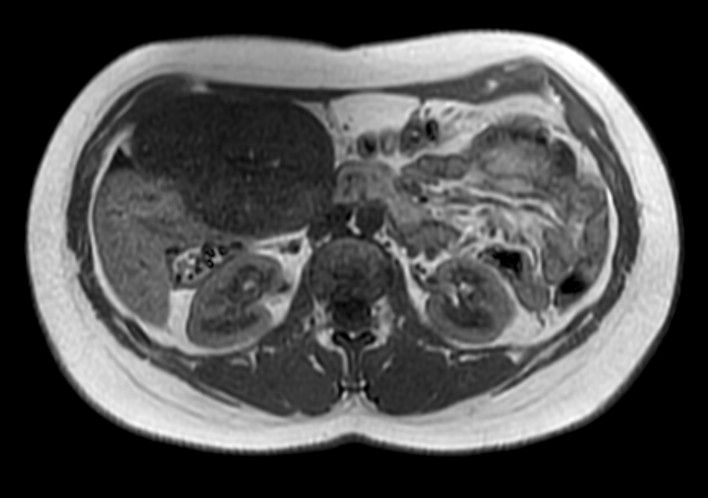
Solid mass measuring 11.3 x 6.8 x 11.0 cm with areas of necrosis and internal hemorrhage in the right abdomen, linked to hepatic segment 5 and receiving its blood supply from the portal and probably arterial hepatic system. Segment 5 shows hyperemia. No evidence of extrahepatic vessel recruitment evident at the resolution of this study. The mass is hypointense to the liver parenchyma on the hepatobiliary phase. Features compatible with parasitic hepatic leiomyoma.
Fatty 9 mm subcapsular lesion at the level of segment 7 - pseudolipoma of the Glisson capsule, most probably.
Solid 7 mm nodule in the left anterior abdomen, either omental or serosal in the wall of the transverse colon - probably a leiomyoma.
Case Discussion
Status post 3 cesarean sections, the latest around 2 months previously. Laparoscopic removal of large fibroid (i.e. leiomyoma) from the anterior uterine wall 5 years previously, removal of several fibroids during a C-section one year later. The latest surgical report (C-section) described a uterus with many fibroids and numerous lesions in the omentum and on bowel loops. Several lesions from the uterus and the omentum were sampled and found to be fibroids on histopathology. Known large exophytic liver mass, suspicious for leiomyoma, but as yet not characterized. Candidate for removal of leiomyomas, working diagnosis of disseminated peritoneal leiomyomatosis.
MRI pelvis and abdomen confirmed the diagnosis and raised the possibility of several pelvic endometriomas among the numerous rectouterine pouch leiomyomas. Of special interest, the MRI study also confirmed that the large exophytic hepatic mass was indeed a parasitic leiomyoma, later verified on histopathology.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.