
Presentation
Recent fall with left knee pain. Incidental finding.
Patient Data
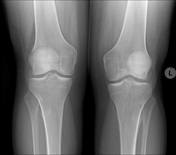
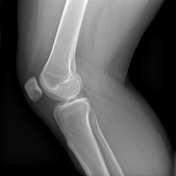

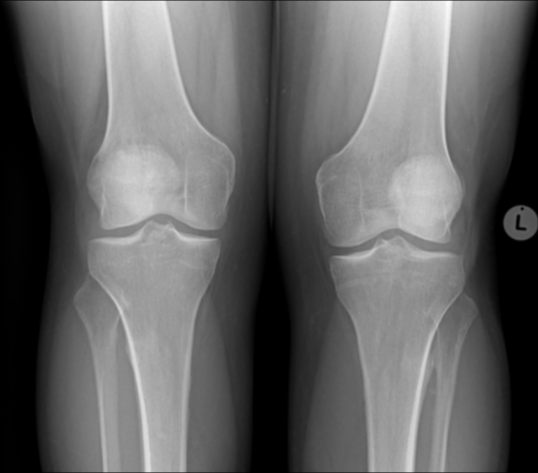
There is minimal medial joint space narrowing bilaterally, plain films are otherwise normal with no fractures, dislocations and no subluxations in view of trauma and blunt impact to the left knee.
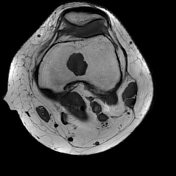

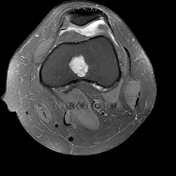
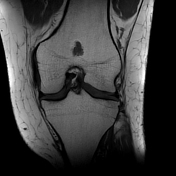

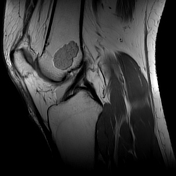

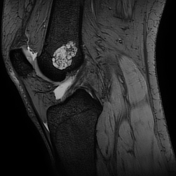
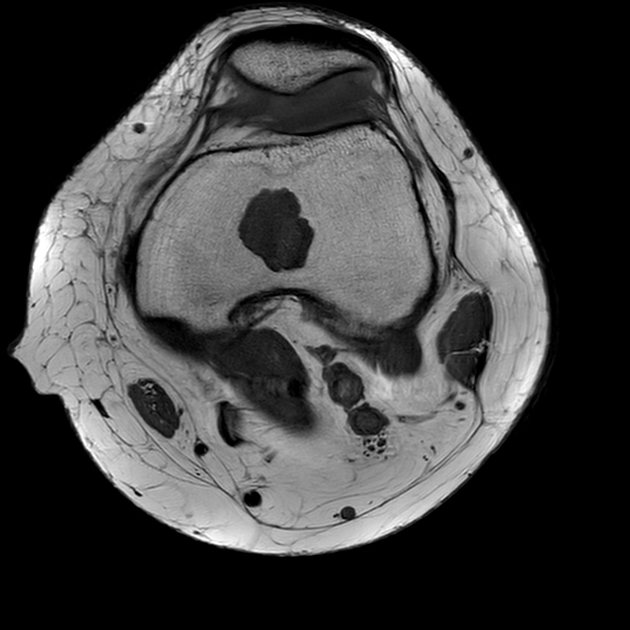
There is an incidental, lobulated, intra-osseous lesion within the distal left femoral shaft with a narrow zone of transition and absence of any perilesional oedema. The centrally located lesion straddles the meta-epiphyseal junction and measures 2.1 x 3.1 cm. It appears T1 hypointense and T2 hyperintense with 'internal rings and arcs' suggesting a chondroid matrix. The spoiled T2* sequence (M-FFE) accentuates the chondroid matrix significantly.
There is no cortical involvement, no endosteal scalloping, no soft tissue involvement or extension, and no periosteal reaction on MRI. There is no pathological fracture.
There is minimal pre and infrapatella soft tissue oedema. The quadriceps and patella tendons are intact with no extensor mechanism injury. There is lateral facet chondromalacia.
The medial and lateral patella femoral retinaculum and patellofemoral ligaments are intact. There is mild supra, retropatellar and intra-articular effusion.
The ACL and PCL are normal. The medial and lateral collateral liagments and ileotibial band are intact. There are no meniscal tears or parameniscal cysts. There are no bone contusions in view of blunt impact to the knee.
Case Discussion
The incidental left femoral lesion has well identified chondroid matrix accentuated by the spoiled T2* sequence. The differential diagnosis includes an enchondroma and a low-grade chondrosarcoma. These 2 lesions are difficult to differentiate due to similar imaging and histological appearances. Due to the absence of aggressive features and a completely asymptomatic patient (he presented due to a fall) and based on the benign imaging characteristics, the lesion was clinically assessed as an enchondroma and a short-term clinical and imaging follow-up was recommended.
The lesion is amazingly poorly identified on the plain films which were done after the MRI.
Case assistance courtesy: Dr DH Jogi.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.