
Presentation
Patient with metastatic cholangiocarcinoma presenting with altered mental status. Hypotensive and tachycardic, febrile at 38.5C. Systolic murmur, lower extremity petechiae.
Patient Data
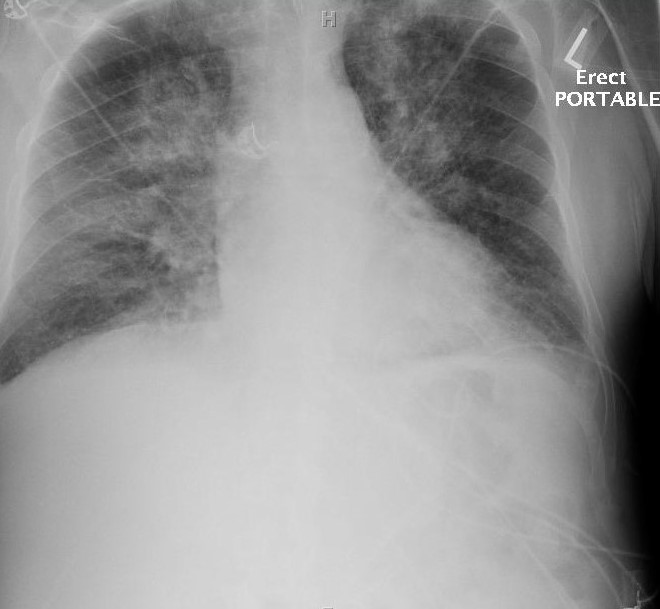
AP portable chest radiograph. Diffuse bilateral perihilar pattern of septal thickening and patchy coalescing airspace opacities. Peripheral Kerley B like lines of right upper lung zone. Pulmonary vasculature is distended and indistinct.
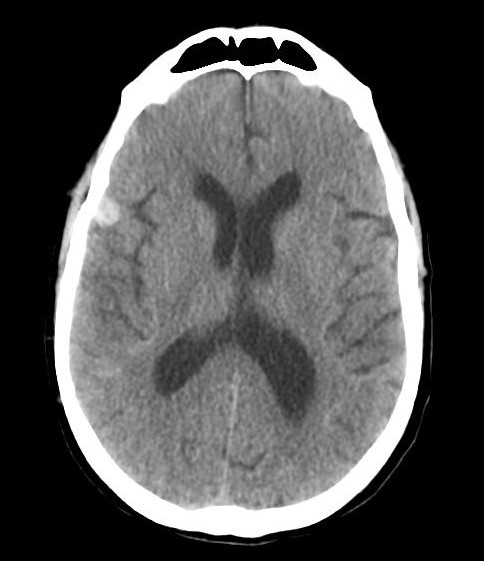
11 mm x 9 mm x 12 mm hyperdense area centred within the far anterolateral extent of the right Sylvian fissure consistent with subarachnoid haemorrhage.


Transthoracic echocardiogram: hyperdynamic left ventricular systolic function with an estimated ejection fraction between 65-70%. Severe left atrial enlargement. Moderate aortic regurgitation, severe mitral regurgitation. Mitral valve leaflets thickened. Oscillating, irregular, hyperdense mass on anterior leaflet consistent with vegetation. Intermittent appearance of mobile echodensity primarily in diastole on the upstream (ventricular) aspect of the aortic valve.
Case Discussion
Blood cultures were drawn and patient was treated for presumptive infective endocarditis. Two cultures resulted positive for viridans group streptococci. Transoesophageal echocardiography was considered but ultimately decided against in alignment with patient's goals of care.
Infective endocarditis describes a bacterial or fungal infection of the endothelial surface of the heart, typically occurring secondary to bacteraemic seeding of an abnormal valve 1. It is distinct from marantic, or nonbacterial thrombotic, endocarditis by the presence of microorganisms within the characteristic vegetations. Echocardiographic features consistent with endocarditis include 2:
- an oscillating, intracardiac mass implanted on a valve or subvalvular apparatus, involving prosthetic material, or on endocardium in the path of a regurgitant jet
- presence of an intracardiac abscess
- new dehiscence of a prosthetic valve
- new valvular regurgitation
The diagnosis is typically made by satisfying the Duke Criteria. Transoesophageal echocardiography is superior to the transthoracic approach for diagnosis and detection of complications; the latter is often useful for patients at low risk and with a low clinical suspicion.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.