
Presentation
Pelvic pain with bowel habit change. Dyschezia. Secondary amenorrhoea. ?DIE on ultrasound with bowel nodule.
Patient Data
ARGANZ Endometriosis MRI Case 3.3



ANTERIOR COMPARTMENT:
Urinary bladder: Normal.
Ureters: Normal.
Vesicouterine pouch: Normal.
Vesicovaginal septum: Normal.
MIDDLE COMPARTMENT:
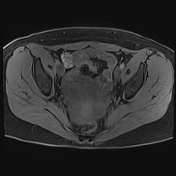
Uterus: Anteverted. 89 mm long with normal morphology. Endometrium 7 mm thick and regular.
No endometrial lesion. No junctional zone thickening. Lower anterior segment caesarean
section scar. Anterior midbody intramural 7 mm T2 dark circumscribed mass, FIGO type 4
fibroid.
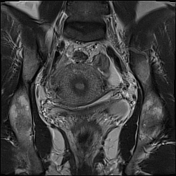
Ovaries: Suspended within simple Pouch of Douglas free fluid, no endometrioma.
Fallopian tubes: No haemato- or hydrosalpinges.
POSTERIOR COMPARTMENT:
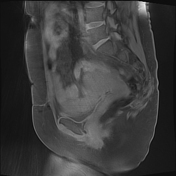
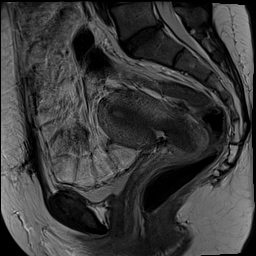
Rectosigmoid colon: At 140 mm from anal opening, the Pouch of Douglas is obliterated by a
T2 dark fibrotic linear bands. There is adjacent subtle upper rectal 35 mm x 10 mm anterior
mural thickening, correlates to the typical mushroom-shaped lesion seen on a prior ultrasound. This is separate to the right uterosacral ligament on MRI. No second bowel lesion.
Pouch of Douglas: Obliterated.
Torus uterinus: Fixed to upper rectum.
Uterosacral ligaments: The nodularity seen on a prior ultrasound is not confirmed on MRI.
Rectovaginal septum: Normal.
INCIDENTAL FINDINGS: None.
Case Discussion
Posterior compartment endometriosis with obliterated Pouch of Douglas. Extensive T2 dark
linear superficial bands with subtle upper rectal thickening correlates to a typical mushroom-shaped lesion on ultrasound.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.