
Presentation
Endometriosis with bowel adherent at the vault. Worsening pain and bowel symptoms.
Patient Data


ANTERIOR COMPARTMENT:
Vesicouterine pouch: normal.
Vesicovaginal septum: normal.
Urinary bladder: normal.
Ureters: normal.
MIDDLE COMPARTMENT:
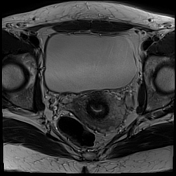
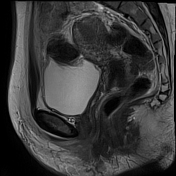
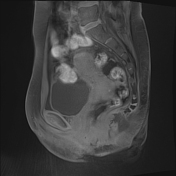
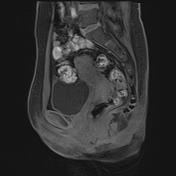
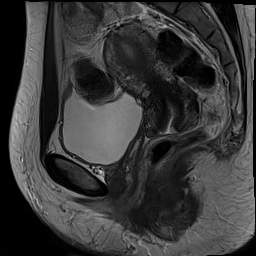
Uterus: Anteverted 89 mm long. Endometrium 10 mm thick and regular. Thickened junctional
zone, 12 mm posteriorly consistent with adenomyosis. Normal mobility anteriorly, at the fundus but fixed at the posterior cervix.
There is posterior vagina vault 22 x 9 mm T2 dark deep infiltrating endometriosis fixed to the
mid rectal lesion.
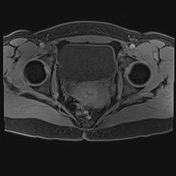
Ovaries: normal.
Fallopian tubes: normal.
POSTERIOR COMPARTMENT:
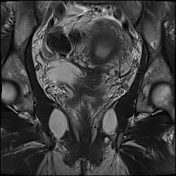
Rectosigmoid colon: At 110 mm from the anal opening there is a 20 x 9 mm mushroom shaped bowel endometriosis fixing the rectum to the vault.
Pouch of Douglas: Obliterated.
Torus uterinus: normal.
Uterosacral ligaments: normal.
Rectovaginal septum: normal.
INCIDENTAL FINDINGS: None.
Case Discussion
Endometriosis. Predominantly mid and posterior compartment. Rectosigmoid colon is involved
with rectal endometriosis obliterating the pouch of Douglas and fixing to the posterior vault/torus
deep endometriosis. Typical butterfly-shaped symmetric lesions.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.