
ERCP for pancreatic cancer complicated by perforation of pharyngeal pouch
Presentation
2 months of malaise, weight loss and more recently, jaundice.
Patient Data


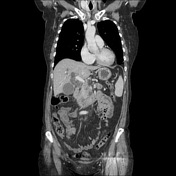
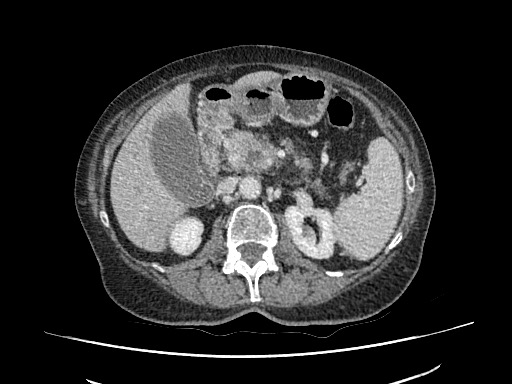
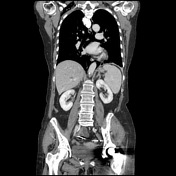
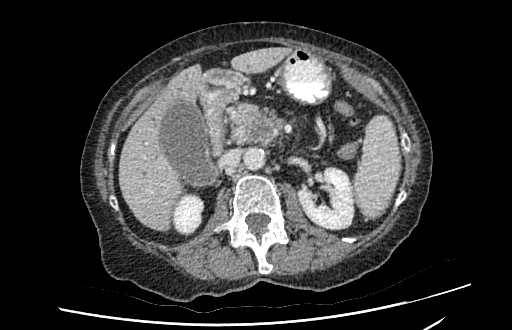
Ill-defined mass centered on the pancreatic head with pancreatic duct, intrahepatic and extrahepatic duct dilatation. Ill-defined low attenuation lesion in segment VII of liver in keeping with metastasis. Dilated gallbladder. Local lymphadenopathy.
An ERCP was planned in order to obtain histological tissue and to stent the bile ducts to relieve the jaundice. However, esophageal intubation was difficult with a pharyngeal pouch encountered and the patient experienced severe chest pain during the procedure so it was abandoned.
Chest & soft tissue neck XR


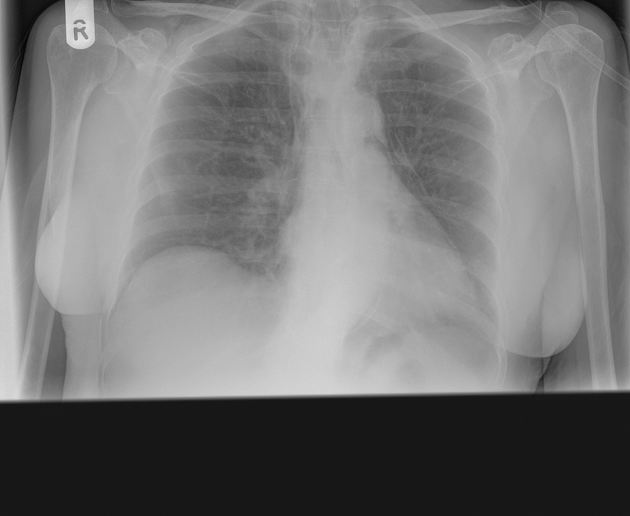
Signs of pneumomediastinum with gas extending into the soft tissues of the neck.
A CT with oral contrast was requested to confirm a perforated pharyngeal pouch.
CT with oral contrast

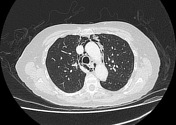
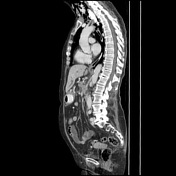
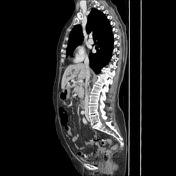
100 ml of 5% Gastrografin was administered immediately before scanning. There is a large pharyngeal pouch filled with oral contrast, with leak from the left anterior aspect into the adjacent soft tissues, where there is also a large volume of gas. Extensive soft tissue emphysema and pneumomediastinum. No pneumothorax. No change in appearances of pancreatic mass.
Case Discussion
Painless jaundice is highly suspicious for pancreatic malignancy, and in this case leads to the double duct sign. One of the known complications of endoscopy is perforation of a pharyngeal pouch which, in this case, was not previously known. Oral contrast administration in CT can be helpful in detecting the site of perforation.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.