
Presentation
Presenting with pleuritic chest pain, hypoxia - desaturating to 70% (baseline 85%), sinus tachycardia (HR to 130). History of congenital heart problem and recent cardiothoracic surgery.
Patient Data






Standard CTPA protocol.
Fontan fenestration procedure and a Bidirectional Glenn procedure were done for univentricular congenital heart disease in childhood. Recently, Damus Kay Stansel operation and Fontan fenestration closure with epicardial lead attachment was done.
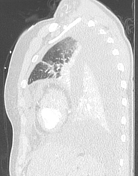
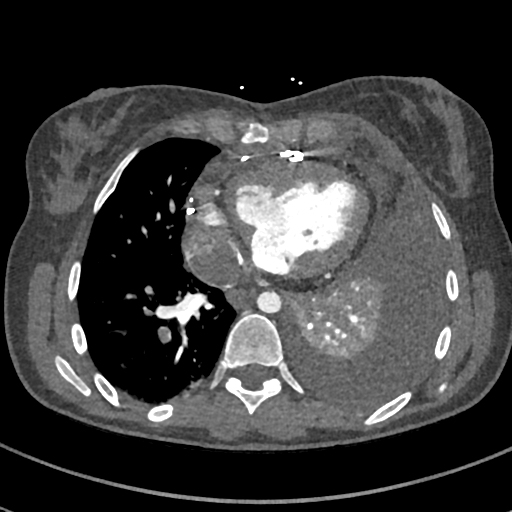
Patent SVC with flow into the pulmonary artery. No contrast is seen in the IVC or right lower lobe pulmonary arteries, right sided PE cannot be excluded. No left-sided PE. Large left pleural effusion with left lower lobe collapse. Small pericardial effusion.
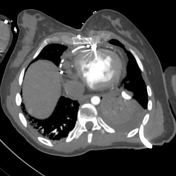





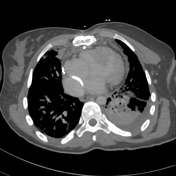
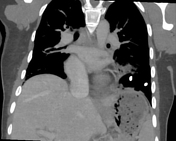

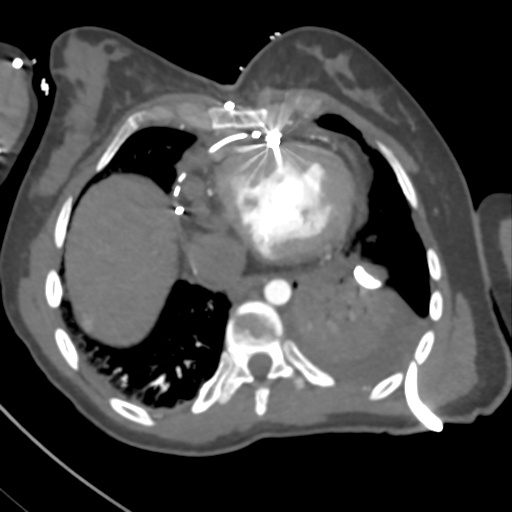
The repeat CTPA was triggered when iodinated contrast was in the aorta. Now multiple filling defects are seen within the right pulmonary artery and segmental branches of the right lower lobe, these findings were reported as consistent with pulmonary emboli. A delayed scan was also performed at 70secs after contrast administration.
A left-sided intercostal catheter has been inserted and the left pleural effusion is reduced in size. There is now left hydropneumothorax with associated left basal collapse/consolidation.
Case Discussion
In childhood the patient had a Fontan fenestration procedure and a Bidirectional Glenn procedure for univentricular congenital heart disease. Due to worsening exertional dyspnea at age 31, the patient received an elective Damus Kay Stansel operation and Fontan fenestration closure with epicardial lead attachment.
A month after the elective Damus Kay Stansel operation and Fontan fenestration closure the patient represented to hospital with chest pain, dyspnea and lightheadedness.
A CT Pulmonary Angiogram (CTPA) was performed to assess for the presence of pulmonary embolism (PE). The initial scan was non-diagnostic. Due to the altered hemodynamics (venous return from the inferior vena cava) there was inadequate contrast in the right sided pulmonary arteries. The decision was made to repeat the CTPA with a slight delay and another scan with a 70 second delay. The repeat CTPA was reported as multiple filling defects in the right pulmonary artery and right lower lobe segmental arteries consistent with PE.
With ongoing discussions with the clinical team, it was felt that PE would be unlikely in a young patient on therapeutic anticoagulation.
The cardiologist then performed a pulmonary angiogram from the right femoral vein in the cardiac catheterization laboratory. No filling defect was seen in the right pulmonary artery or segmental arterial branches. The CTPA was deemed a false positive finding.
A left pleural effusion was also treated with thoracocentesis.
This case highlights the difficulty in obtaining a diagnostic CTPA in patients with Fontan circulation.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.