
Presentation
Shoulder pain, particularly with movement and at night. Difficulties lifting the left arm.
Patient Data




Findings:
Acromioclavicular joint:
- low lying acromion
- small anterior acromial spur
Subacromial-subdeltoid bursa:
- an increased amount of fluid and also fluid within the anterior part of the bursa
Glenohumeral joint:
- mild shoulder joint effusion
Rotator cuff:
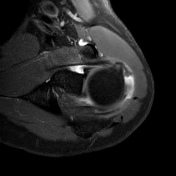
- full-thickness/transmural, U-shaped tear of the distal supraspinatus tendon (10 x 20 mm)
- possible extension into the focally thickened distal superior infraspinatus tendon
- focal high signal within the inferior distal subscapularis tendon
- unremarkable teres minor tendon
Muscles:
- no significant atrophy, negative tangent sign
- no fatty degeneration
Rotator Intervall and long head of the biceps tendon:
- mild linear signal alteration of the suprahumeral part of the long head of the biceps tendon
- normal location/course within the bicipital groove
- some fluid within the synovial sheath
- unremarkable coracohumeral and superior glenoid ligaments
Bones:
erosions/cystic changes of the lateral aspect of the greater tuberosity
Impression:
Rotator cuff tear with medium size full-thickness tear of the distal supraspinatus tendon (Patte grade 1) with extension posteriorly into the superior infraspinatus tendon.
No significant atrophy or fatty degeneration of the muscle.
Tendinosis of the inferior subscapularis tendon.
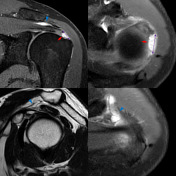
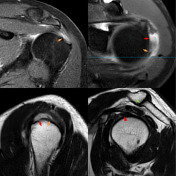
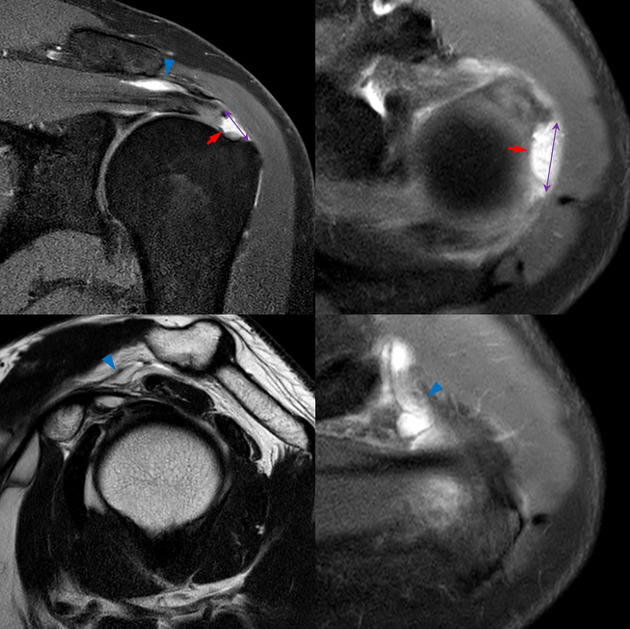
Key findings:
- full-thickness/transmural tear of the distal supraspinatus tendon (red arrow) with increased fluid in the subacromial/subdeltoid bursa (blue arrowhead)
- mediolateral and anteroposterior diameter (purple measurement)
- posterior extension into the anterosuperior part of the infraspinatus tendon (orange arrow)
- mild long head biceps tendinosis (red arrowhead)
- small anterior acromial spur (green arrow)
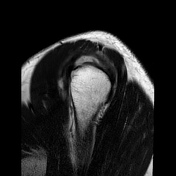
Supraspinatus atrophy and fatty degeneration:
no signs of atrophy
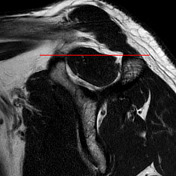
- negative tangent sign: the supraspinatus muscle belly is cut by a tangent from the base of the coracoid process to the superior margin of the scapular spine 7,
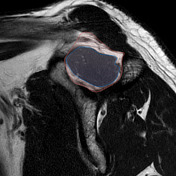
- the cross-sectional area of the supraspinatus muscle (blue) compared to the cross-sectional area of the supraspinatus fossa (red) 1,3,9 is more than 50% in this case
no fatty degeneration as per Goutallier classification 8
Case Discussion
This case illustrates a typical full-thickness rotator cuff tear and discusses findings, which should be included in the radiological report 1-4:
- grading of the rotator cuff tear (full-thickness, partial-thickness) including increased fluid in the subacromial/subdeltoid bursa
- the shape of the rotator cuff tear - important for the selection of the surgical technique 3
- tear dimensions including tendon retraction, Patte classification 6
- tear extension into other rotator cuff muscles or adjacent structures - in this case, the distal infraspinatus tendon
- atrophy assessed by the tangent sign 7 or by cross-sectional area 3,9
- fatty degeneration of the affected muscles (Goutallier classification) 8
- suspected cause or mechanism of the rotator cuff tear including signs of impingement, decreased acromiohumeral distance, tendon degeneration, glenohumeral instability
- other findings e.g. calcific tendinitis or excessive cystic change/erosions of the greater tubercle could affect surgical repair


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.