
Presentation
2 months of the left sided hemiparesis treated as a stroke.
Patient Data
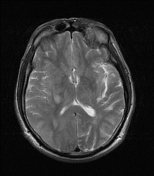

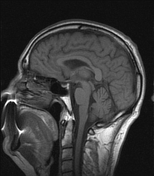
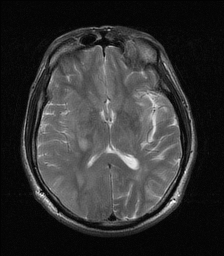
Irregularly shaped mass involving both right pre/postcentral gyri with inhomogeneous inner architecture.
Mild vasogenic oedema, mild mass effect to the right ventricle.
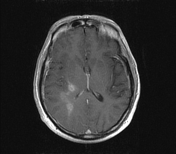
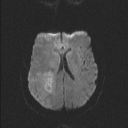
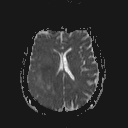
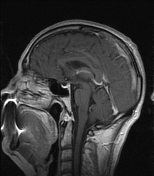
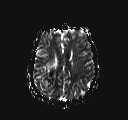
Vivid enhancement elevated CBV and CBF and diffusion restriction of the solid component.
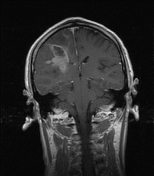
The right proximal portion of corticospinal tract fibres involved, best seen on the post contrast coronal images, at the level of tentorium cerebelli.
Case Discussion
This case well demonstrates how glioma cells can migrate along myelinated white matter tracts and also shows an important role of MRI examination among patients with a possible stroke signs.
A primary brain tumour is one of the several clinical presentations for a 'stroke mimic'.
Note: As this case does not provide a histological diagnosis of IDH mutation status, according to the current (2016) revision WHO classification of CNS tumours this tumour would be classified as a probable glioblastoma NOS.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.