
Hepatocellular carcinoma containing microscopic (intracytoplasmic) fat
Presentation
Suspicion of cirrhosis on ultrasound. MRI evaluation recommended.
Patient Data
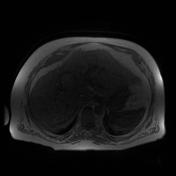

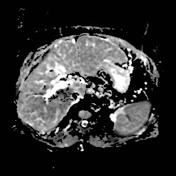

There are many stigmata of cirrhosis in this patient : micronodular liver contours & parenchyma, relative hypertrophy of the left liver lobe, dilated portal vein, splenomegaly, permeable umbilical vein, etc. Minimal ascites surrounds the periphery of the liver.
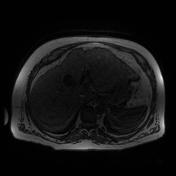
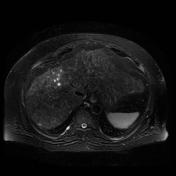
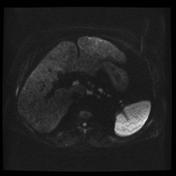
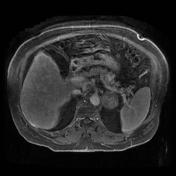
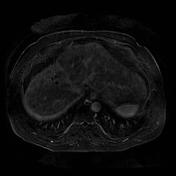
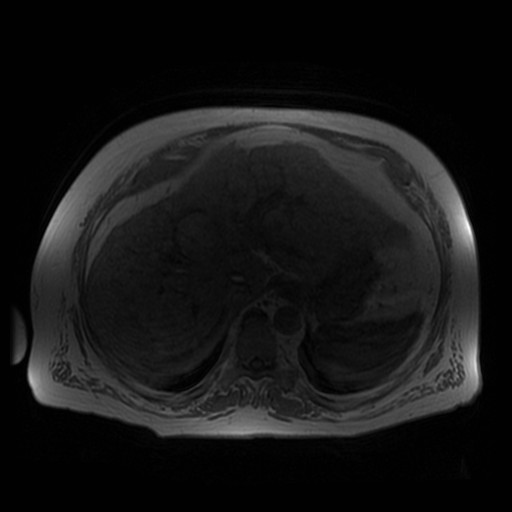
MRI shows a mass occupying the 8 & 4A liver segments, iso-intense on T2WI - slightly hyperintense on T1WI (in-phase). There is an important drop of signal on in and out of phases images, compatible with microscopic fat (intracytoplasmic). The mass only enhances peripherally on all T1C+ images, including delayed images at 30 minutes. The mass is responsible for a focal upstream dilatation of intra-hepatic bile duct. Considering the cirrhosis stigmata, the most probable diagnosis is hepatocellular carcinoma until proven otherwise. Peripheral cholangiocarcinoma are not known to contain microscopic fat. Other fat containing lesions are highly improbable.
There is a siderotic nodules located in segment 7 (hypo-intense T1 & T2, non enhancing).
Left adrenal adenoma with cystic component, otherwise typical (50 % washout, signal drop on in & out of phase, etc.).
Case Discussion
Histological diagnosis of HCC was confirmed. This is a unusual case of HCC containing microscopic fat (signal drop on opposition phase images). In cirrhotic patient, more than 80 % of microscopic fat containing lesions are malignant, most of which are HCCs.
The differential diagnosis of fat containing liver lesions includes :
Benign:
- focal fatty change (focal steatosis)
- adenoma
- FNH
- lipoma
- angiomyolipoma
- cystic teratoma
- cystic adrenal rest tumor
- pseudolipoma of the Glisson capsule
- xanthomatous lesions in Langerhans cell histiocytosis (LCH)
Malignant:
- HCC
- metastastic liposarcoma
- primary liposarcoma
- other fat containing liver metastases


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.