
Presentation
The patient has a history of congenital uterine anomalies and has undergone two cesarean sections, with a history of a severe gynecological infection.
Patient Data
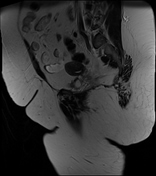

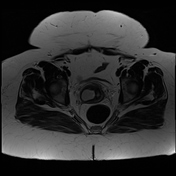
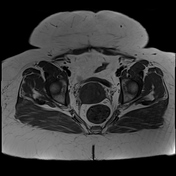
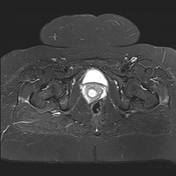
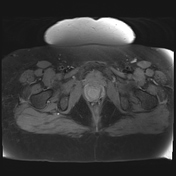
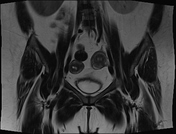
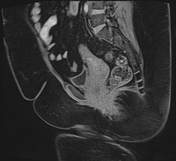
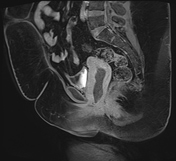
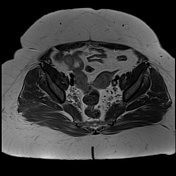
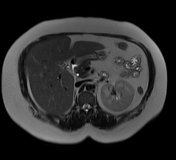
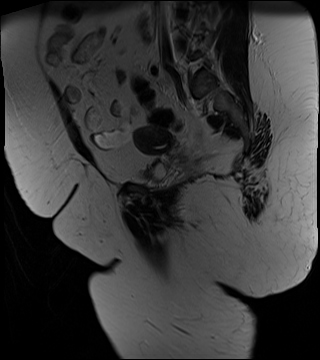
Two widely divergent uterine horns are seen, showing an external fundal contour with cleft dipping >1 cm; dividing the uterine corpus and cervix completely into two endometrial cavities, two cervices, and two vaginal cavities; consistent with a didelphys uterus.
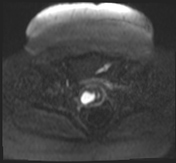
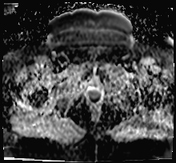
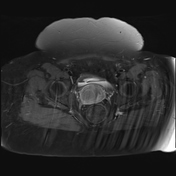
The upper two-thirds of the right hemi-vagina is markedly distended and contains fluid content, demonstrating intermediate signal intensity on T1-weighted images (WIs) and mixed intermediate and bright signal intensity on T2 WIs (shading). (Obstructed right hemi-vagina likely due to the presence of vaginal septum).
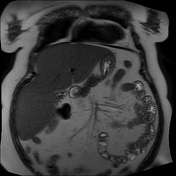
The right kidney is absent. (Ipsilateral renal agenesis).
A solitary hypertrophied left kidney is observed.
Multiple gallbladder stones are observed.
Case Discussion
Herlyn-Werner-Wunderlich (HWW) syndrome is a rare congenital malformation also known as OHVIRA-Syndrome (Obstructed hemi-vagina and ipsilateral renal anomaly).
It is a congenital development anomaly of the paramesonephric (Müllerian) and mesonephric (Wolffian) ducts.
Our case showed a classic diagnostic triad of uterus didelphys, a double vagina with one obstructed hemi-vagina, associated with ipsilateral renal agenesis. Other urinary developmental malformations such as multicystic dysplastic kidney and renal duplication have also been reported in similar cases.
According to various classification systems for Müllerian duct anomalies, OHVIRA syndrome is classified under class III in the ASRM classification and class U3b C2 V2 in the ESHRE classification.
Our case falls under U3b C2 V2, which is characterized by a complete bi-corporeal uterus, a double "normal" cervix, and a longitudinal obstructing vaginal septum, along with a partial type of obstruction (class 2.1), indicating an underlying possibility of partial resorption of the vaginal septum and communication between the two vaginae.
The main complaints in our case included vaginal secretions and recurrent genital infections. The patient also experienced delayed presentation and a late age of onset, likely due to partial genital outflow obstruction.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.