
Presentation
History of breast cancer and metastasized uterine sarcoma. CT was performed for re-staging.
Patient Data



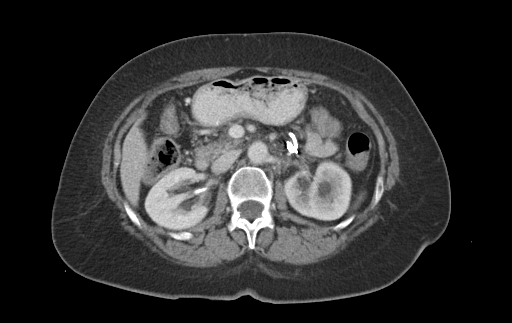
The inserted ureteric stent on the left side is displaced cranially of the renal pelvis as the proximal ureter is ruptured due to stent placement. However, there is no sign of urinoma or ascites. There is associated grade 1 obstructive uropathy.
There is thickening of the left ureter, consistent with tumorous infiltration s/p resection of a uterine sarcoma. There is a suspect mass (5.6 x 5.4 x 5.0 cm) between the left common iliac artery and the iliopsoas muscle, consistent with lymph node metastasis. The lumbar plexus appears to be infiltrated.
There is also a hypodense cortical mass of the mid-level of the right kidney which required further imaging.
Case Discussion
Ureteric rupture is a rare condition and mostly traumatic due to iatrogenic trauma (as in this case) or penetrating or blunt trauma. Nontraumatic ureteric rupture is even less common and is usually caused by increased intraureteric pressure due to a distal obstruction, e.g. ureteric stones, suture material, obstructive abdominal or pelvic mass.
While a lot of urogenital imaging is performed using excretory urography, computed tomography allows a more detailed diagnosis of ureteric rupture. Especially imaging during the delayed secretory phase can help detect even small ureteric leaks.
This is an interesting case as the patient did not complain about a sudden onset of abdominal pain and no urinoma or other free abdominal fluid was present while gross displacement of the ureteric stent can be clearly demarcated.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.