
Presentation
Subtle deviation and decreased volume of the tongue on the right side from 18 months ago.
Patient Data
Age: 35 years
Gender: Male
From the case:
Isolated hypoglossal nerve paralysis


Download
Info

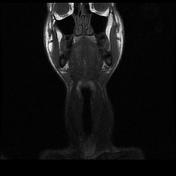
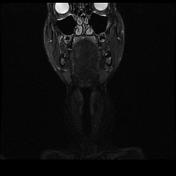
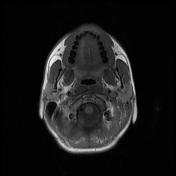
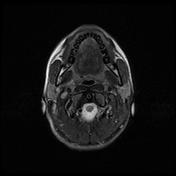
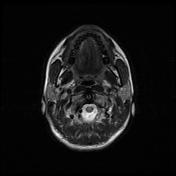
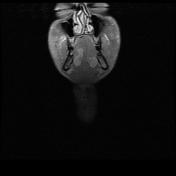
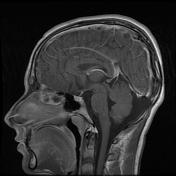
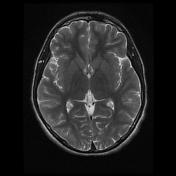
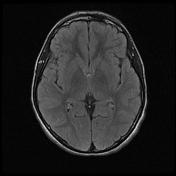
Affected right side of the tongue has a high signal on both T1WI and T2WI due to fatty infiltration as a consequence of longstanding denervation of the hypoglossal nerve.
Right hemiatrophy and deviation of the tongue to the right side.
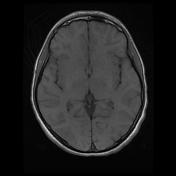
Otherwise head and neck MRI is normal.
Case Discussion
Unilateral atrophy of the tongue is the most important radiologic feature of hypoglossal nerve paralysis. When it is identified, thorough assessment of the hypoglossal nerve from the brainstem to the tongue should be performed.
In acute hypoglossal nerve palsy:
- tongue deviation toward the weak side
- oedematous change (T1WI hypointense, T2WI hyperintense)
In chronic hypoglossal nerve palsy:
- tongue deviation toward the weak side
- tongue atrophy (volume loss)
- fatty infiltration (both T1WI and T2WI hyperintense)


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.