
LAD occlusion with severe acute heart failure and severe generalized atherosclerosis
Presentation
The patient was referred to percutaneous coronary intervention (PCI) due to ST elevated myocardial infarction. During PCI, no access was possible through either limb, suggesting aortic dissection. CTA had been requested.
Patient Data





Enhancing kidneys and contrast excretion due to previous PCI on non-enhanced CT scan.
On ECG-gated CTA, no aortic dissection is present. Generalized severe atherosclerosis is evident:
severe stenosis on both subclavian arteries and brachiocephalic trunk
chronic occlusion at the aortic bifurcation (Leryche -syndrome)
chronic occlusion of superior mesenteric artery
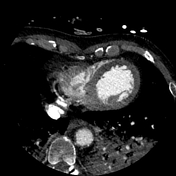
LAD proximal segment occlusion and signs of severe acute heart failure:
LAD proximal segment occlusion
distal enhancement may be due to collaterals
hypodense myocardium (on venous phase) at LAD territory, suggesting myocardial ischemia
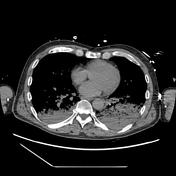
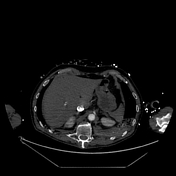
huge amount of intravenous contrast regurgitation into the inferior caval vein.
bilateral alveolar lung edema
regular pulmonary spetal thickening
Signs of aspiration:
intubated
bilateral dorsal/basal consolidations
Case Discussion
CTA confirmed the pretest clinical diagnosis (acute myocardial infarction). This case demonstrates the CTA signs of acute coronary occlusion and its consequences: myocardial ischemia and acute heart failure. The severe, generalized atherosclerosis halted PCI and caused the impression of acute aortic dissection.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.