
Presentation
Left-sided facial droop along with ipsilateral ataxia, Horner syndrome.
Patient Data
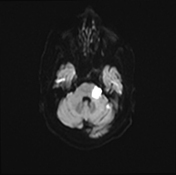

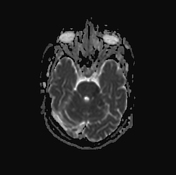
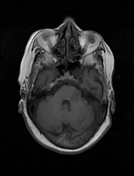
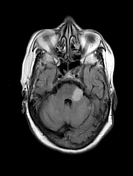
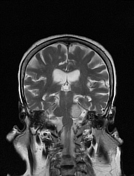
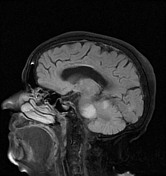
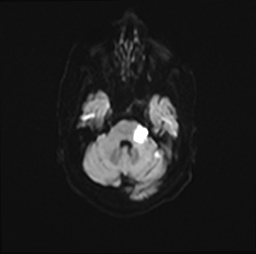
Left lateral pontine and adjacent left middle cerebellar peduncle large patchy lesion of abnormal signal and diffusion characteristics, that elicits hypointensity in T1, hyperintensity in T2 & FLAIR, and markedly restricted in the diffusion eliciting low signal in ADC and high signal in DWI consistent with acute infarction.
Other multifocal infarcts are seen involving bilateral superior cerebellar hemispheres, pons and left medial thalamus eliciting almost similar signal alteration however with variable diffusion criteria, some are acute similar to the left lateral pontine lesion and others are subacute or chronic with less evident ADC hypointensity and DWI hyperintensity.
Bilateral cerebral white matter signal changes related to chronic small vessel disease.
Case Discussion
This case represents the MR picture of a medical condition known as lateral pontine syndrome or Marie Foix syndrome that is caused by occlusion of the perforator branches of the basilar and anterior inferior cerebellar arteries, leading to lateral pontine infarction with subsequent damage of the sympathetic tract as well as various nuclei such as facial motor, vestibular, cochlear, and spinal trigeminal. This results in several symptoms such as ipsilateral ataxia due to involvement of the middle cerebellar peduncle, facial droop, Horner syndrome, hearing loss, loss of pain and temperature sensation of the face, and contralateral loss of pain and temperature of the body due to damage of the spinothalamic tract.
Co- contributors: Dr. Gomaa Abugabal, Azza Ghobashy, Mohamed Ibrahim, Sherif Essam, Ahmed Bakry and the neurology team of Etay Elbaroud hospital, Egypt.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.