
Presentation
Known patient with grade II astrocytoma received several sessions of radiotherapy and on regular follow up.
Patient Data
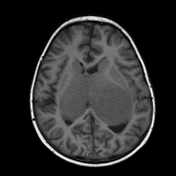

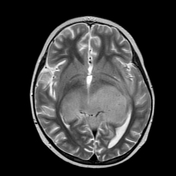
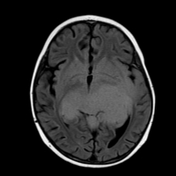
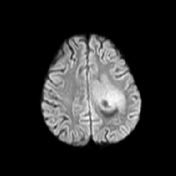
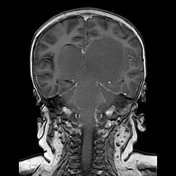
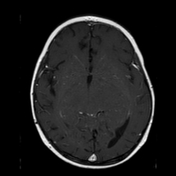
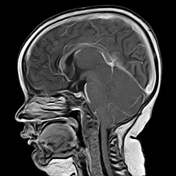
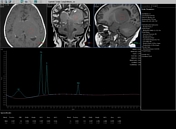
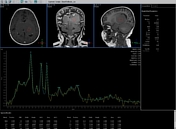
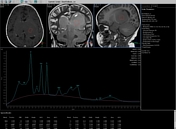
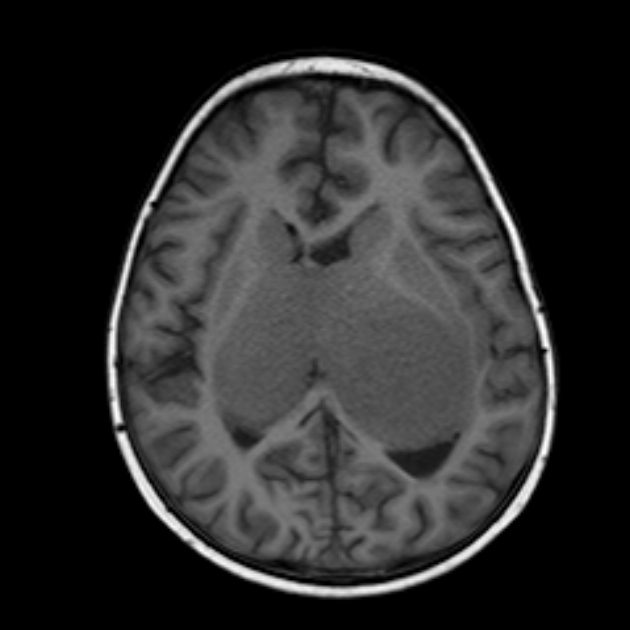
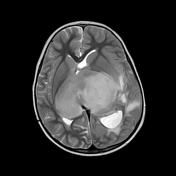
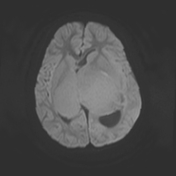
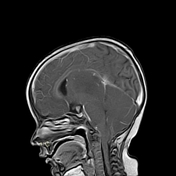
Diffuse enlargement and abnormal signal of both thalami and to lesser extent caudate and lentiform nuclei together with posterior aspect of hippocampus, midbrain tectum and cerebellar vermis. They display bright signal on T2 and FLAIR, iso signal on T1 with no considerable enhancement on post contrast study. DWI reveals an area of faint diffusion restriction on the most superior part of left side thalamic lesion. MRS confirms the neoplastic nature in form of strike elevation of Cho, reduced NAA peak on long echo with marked elevation of mI (Myo-inositol) on intermediate echo. No lipid/lactate peak elevation.
Diagnosis: Diffuse astrocytoma WHO grade II
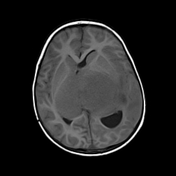
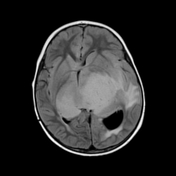
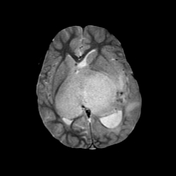
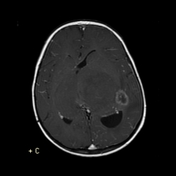
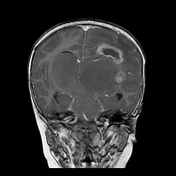
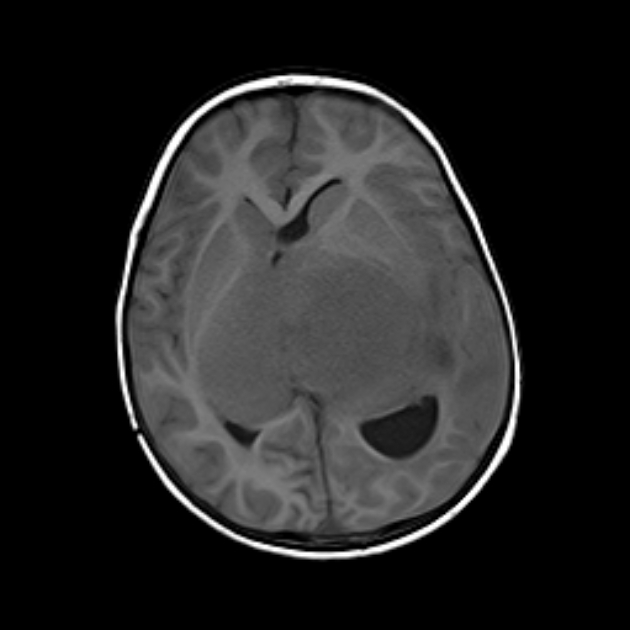
This scan was 6 months after the original scan. Newly developed two suspicious areas at lateral and superior margin of left thalamic lesion. They showed irregular marginal enhancement and surrounded by moderate perifocal oedema. There is associated supratentorial hydrocephalic changes likely from obstructed aqueduct of sylvius. The hypointense signal (blooming) on T2* images were attributed to microhaemorrhage and haemosiderin deposition
Case Discussion
The de novo lesions were suspicious of anaplastic transformation, hence biopsy was taken and confirmed radiation necrosis. DWI allowed early detection of areas of abnormal diffusion few months before the changes were detected on conventional MRI.
Note: IDH mutation status is not provided in this case and according to the current (2016) WHO classification of CNS tumours, this tumour would, therefore, be designated as a diffuse astrocytoma NOS.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.