
Presentation
Longstanding lower pelvic pain.
Patient Data


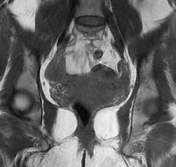
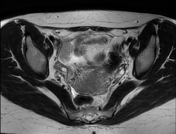
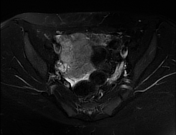

Retroverted uterus with CS niche which shows a small scar of dark signal.
Normal size and signal of both ovaries.
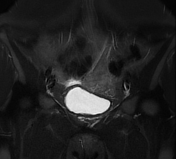
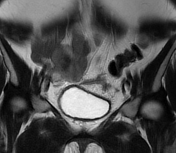
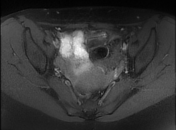
Lower anterior pelvic linear (possibly T shaped) structure evident on the (axial, coronal and sagittal images), surrounded by soft tissue signal of low signal, likely granulation tissue.
Opinion: Lower anterior pelvic extra-uterine T-shaped linear structure surrounded by granulation tissue which was highly suggestive of extra-uterine IUCD migration.

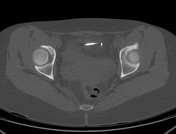
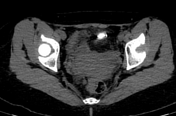


Non contrast CT scan confirmed the extra-uterine location of the IUCD which was seen floating within the anterior aspect of the pelvic cavity, surrounded by fat stranding.
Case Discussion
On MRI, there was a linear T-shaped structure surrounded by low signal intensity granulation tissue which was highly suggestive of IUCD extra-uterine migration.
Non contrast CT scan of the pelvis confirmed this possibility by the presence of the IUCD outside the uterus seen floating within the anterior aspect of the pelvic cavity.
Upon further questioning, the patient reported history of IUCD insertion, yet since a while she stopped to feel the IUCD string and she concluded it probably fell out.
Though in this case, the IUCD had perforated the uterus and migrated anteriorly within the pelvic cavity.
IUD perforation is ranging from embedment in the myometrium to complete transuterine perforation and migration of the IUD into the peritoneal cavity.
Embedment: refers to IUD penetration into the endometrium or myometrium without extension through the serosa.
Intraabdominal migration occurs when the IUD is freely floating in the abdomen or pelvis, encased in adhesions, or adherent to bowel or omentum. Adhesions can lead to infertility, chronic pain, and intestinal obstruction.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.