
Presentation
Chronic obstructive pulmonary disease (COPD) exacerbation.
Patient Data


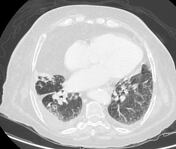

Right upper lobe (RUL) consolidation with air bronchogram. Enlarged lymph nodes in several mediastinal stations, slightly larger compared to previous study from 4 years earlier (not shown). Mildly enlarged bihilar lymph nodes. Diffuse bronchial wall thickening. Bilateral pleural effusion - small on the right and tiny on the left.
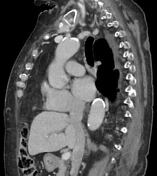
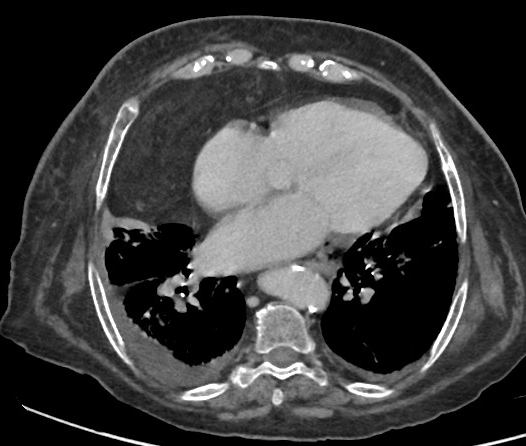
Greater omentum herniates into the right cardiophrenic angle through anterior midline diaphragmatic hernia (Morgagni hernia) with 6.6 cm wide neck, compressing the right lung, evident as atelectasis abutting the herniated omentum in the right upper and middle lobes.
Dilated pulmonary trunk and main pulmonary arteries.
Calcified root of aorta, LAD and LCx.
Bilateral subscapular elastofibroma dorsi.
Rounded cutaneous lesion right of midline at level of T4-T5.
Case Discussion
History of chronic obstructive pulmonary disease (COPD) and obesity hypoventilation syndrome (OHS), on BiPAP and oxygen therapy. Past heavy smoker.
Hospitalised due to COPD exacerbation.
Large Morgagni hernia with herniated omentum compressing the right lung.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.