
Presentation
Severe headache and stroke-like episode
Patient Data
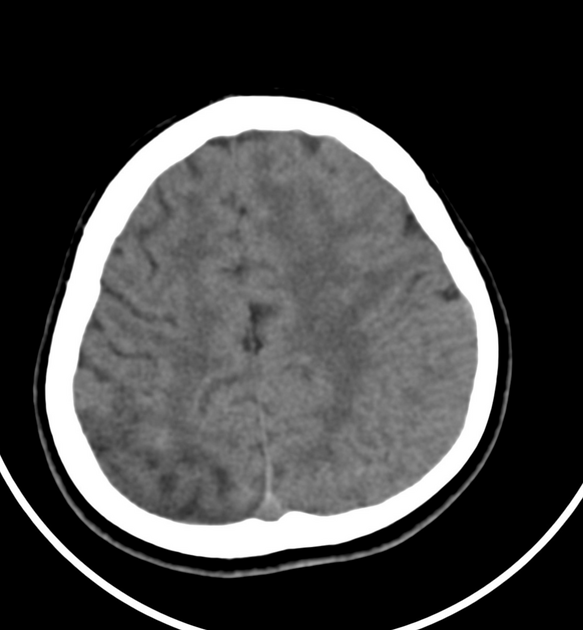
attenuated ventricular system
no midline shift
There is right tempro-parietal cortical/subcortical heterogenous mostly hypodense area with ill-defined cortical linear hyperdensity and prominent cortical sulci suggesting ischaemic changes with cortical laminar necrosis
No definite intra or extra-axial areas of recent blood density

attenuated ventricular system
no midline shift.
-
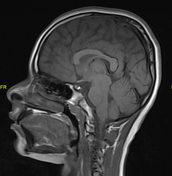
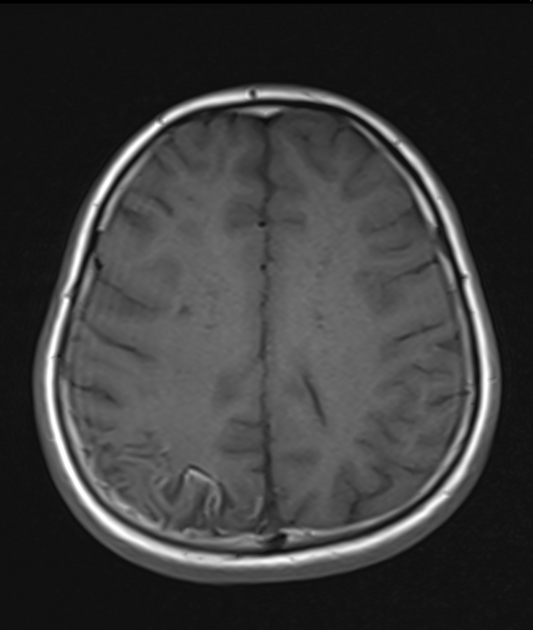
T1:
-
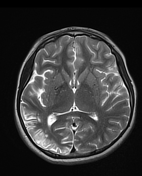
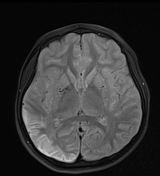
T2/FLAIR
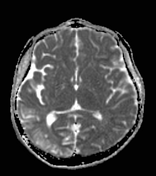
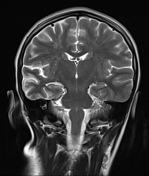
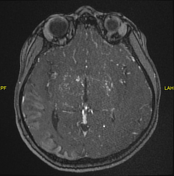
right tempro-parietal cortical/subcortical high signal intensity (axial T2, coronal T2 and axial FLAIR)
the lenticulostriate collaterals appear as multiple flow voids piercing the basal ganglia (axial T2, axial FLAIR) and replacing the M1 segment of MCA (axial T2)
Also, there is bilateral FLAIR high signal intensity at the sulci suggesting "Ivy sign"
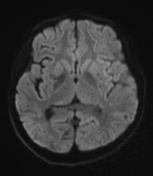
DWI/ADC: free restriction.
-
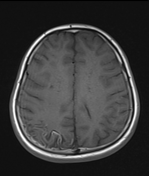
T1 C+
right temporoparietal cortical enhancement with free restriction suggesting subacute infarction due to destruction of blood brain barrier
numerous collaterals at the basal ganglia and replaced the proximal MCA on both sides
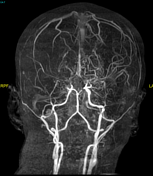
MRA revealed, severe narrowing and tapering of distal ICA on both sides. Occluded MCA on both sides and replaced by numerous collaterals
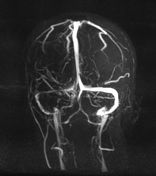
MRV revealed hypoplastic right transverse and sigmoid sinuses
Case Discussion
The characteristic narrowing of the supraclinoid internal carotid arteries and circle of Willis vessels with extensive small collateral arterial networks evolving from the lenticulostriate are highly suggestive of moyamoya disease.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.