
Presentation
A prodrome of flu-like symptoms consisting of a fever, sore throat, fatigue, rhinitis and night sweats. 1 week later he developed a painless, non-pruritic, generalised rash.
Patient Data
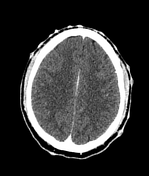

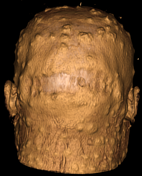

There are extensive, superficial, scalp and facial soft tissue, enhancing papules and vesiculo-pustules of varying sizes. There are no superficial drainable abscesses, and no osteitis or cranial osteomyelitis.
Extensive bilateral solid, non-necrotic IIa, IIb, Va and Vb lymph nodes are present.
Incidental uncomplicated chronic maxillary antral sinusitis.
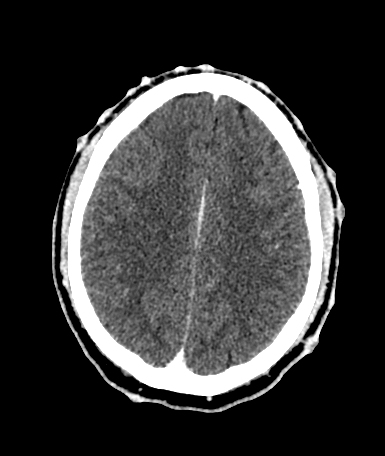
Contrast-enhanced CT brain is otherwise normal.
Specifically, there is no premature involution to suggest HIV encephalopathy, there is no evidence to suggest opportunistic intracranial sepsis in a setting of immune suppression.
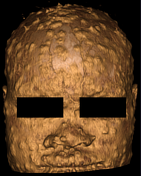
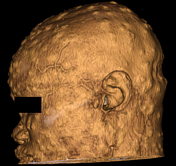
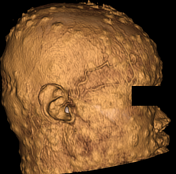
A 3D rendition of the cutaneous papules and vesicular pustules of varying sizes is demonstrated. The 3D image is quite dramatic due to the extensive presentation of the rash involving the scalp and facial soft tissues, in comparison to the mild involvement of the trunk, limbs, and anorectal soft tissues on direct clinical assessment, and CT imaging.







Extensive predominantly solid CT significant and insignificant thoracoabdominal lymphadenopathy. Specifically, pre-tracheal, retrosternal, paratracheal, bi-hilar, bi-axillary, porta hepatic, paravertebral, periaortic, intrapelvic, and inguinal lymphadenopathy.
Features suggestive of post-pulmonary tuberculosis, with multifocal nodules and tree-in-bud appearance. There are no pulmonary cavities, no dense collapse, and no pleural effusions.
There is evidence of hepatosplenomegaly, the liver measures 22 cm craniocaudally and the spleen measures 13.2 cm. There are no hepatic or splenic microabscesses. There are no ascites.
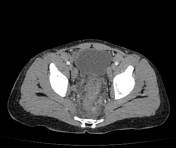
There is evidence of rectal colitis/proctitis with rectal thickening, mesorectal stranding and oedema, and regional lymph adenopathy.
Scattered cutaneous mildly enhancing soft tissue nodules extending from supraclavicular to pelvis. These appear less exuberant than the scalp lesions. There are no drainable superficial soft tissue abscesses.
The thoracic and lumbosacral spine including bony pelvis appear intact and normal with no evidence of tuberculous spondylitis.
CT imaging is otherwise normal.
Case Discussion
A confirmed case of Mpox in a newly diagnosed HIV-positive patient. The patient presented with a prodrome of flu-like symptoms and subsequently developed an extensive rash consisting of papules, and vesicular pustules on the face, scalp, trunk and limbs. The scalp and face were significantly involved (see 3D reformats), with fewer lesions on the limbs and trunk. The skin lesions also involved the oral mucosa, the anogenital region, and the palms and soles of the feet. There were no deep tissue lesions or cutaneous abscesses on CT imaging.
There were no ophthalmological complications clinically.
The CT imaging of the thorax suggested post-primary tuberculosis in a newly diagnosed HIV-positive patient, however, the work-up for TB proved negative, and further investigations were ongoing with a planned follow-up CT scan.
There is significant, solid, generalised lymph adenopathy as demonstrated above. A solitary necrotic lymph node was detected in the right groin. This is a non-specific finding in general, however quite extensive within the axillae, intra-abdominal and groin in this patient. Except for these findings, there are no features of abdominal tuberculosis.
The patient confirmed anorectal pain and discomfort consistent with the CT-identified proctitis, which is present in 14-36% of Mpox patients 2,3.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}