
Presentation
History of a surgical eye procedure 10 years ago, presenting with left periorbital pain, swelling, and discharge. The patient had similar symptoms 6 months prior, which resolved with a course of oral antibiotics.
Patient Data



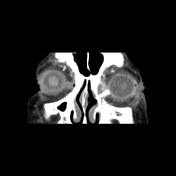
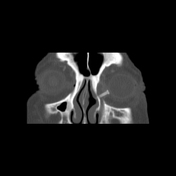
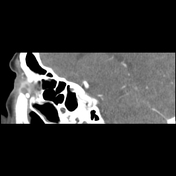

Tubular radiodensity extending from the inferomedial aspect of the left orbit into the middle turbinate of the left nasal cavity.
Rim-enhancing fluid collection in the region of the left nasolacrimal sac.
Left preseptal fat stranding.
Hypoplastic maxillary sinuses.
Case Discussion
The patient had a left nasolacrimal tube which was complicated by dacryocystitis, medial canthal abscess, and preseptal cellulitis. The patient underwent incision and drainage of the abscess and antibiotic treatment with improvement of symptoms.
Nasolacrimal duct obstruction may be congenital or acquired. Acquired obstruction may be primary/idiopathic or secondary. Most often, it is secondary to inflammation/infection of the nasolacrimal duct system (dacryocystitis).
Dacryocystorhinostomy (DCR) surgically bypasses the nasolacrimal duct and is the primary treatment for nasolacrimal duct obstruction. If unsuccessful, a nasolacrimal stent or tube can be used to drain the tears from the eyes to the nose 1, 2, 3. Complications of stents include prolapse/displacement of the stent, granuloma formation, creation of a false passage, and infection.
Case co-authors: Delia Shaher, BS (Stritch School of Medicine); Paul de Bustros, MD (Loyola Department of Ophthalmology)


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.