
Presentation
Past history of head and neck trauma many years ago without seeking medical advice. Now with spontaneous and sudden onset neck pain.
Patient Data


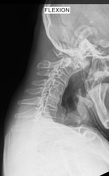


Lateral cervical spine x-ray demonstrates an odontoid fracture and there is significant anterior translation of C1 relative to C2, leading to spinal canal narrowing at this level. Furthermore, the interspinous distance between C1 and C2 is increased. No dynamic instability was demonstrated on flexion and extension lateral radi


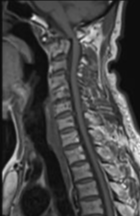

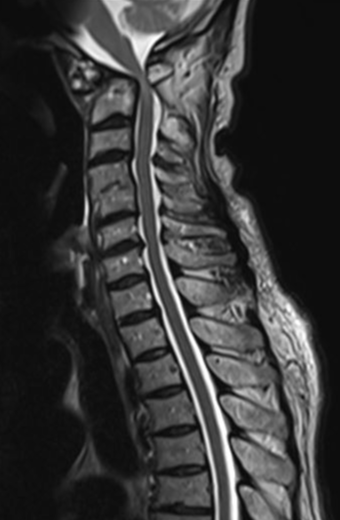
Old dens fracture with anterior displacement of C1 over C2, resulting in significant spinal canal narrowing at this level. There is notable T2 hyperintensity within the spinal cord, suggestive of compressive myelopathy.
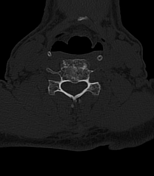


Well-corticated old dens fracture with anterior subluxation of C1 on C2, resulting in spinal canal narrowing. Due to technical limitations, the sagittal stack is not available.

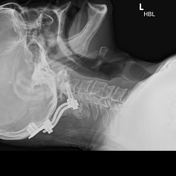
Skull callipers used to stabilise odontoid fracture in orthopaedic ward while awaiting surgical intervention.


Cervical spine x-ray demonstrates postoperative fixation with occipitocervical instrumentation, stabilising odontoid fracture.
Case Discussion
Type II odontoid fractures frequently go into nonunion and undiagnosed odontoid fractures may lead to chronic C1–C2 instability and progressive myelopathy. A conservative approach is recommended for older patients with stable, non-progressive C1–C2 deformity 1.
Preoperative traction is a reasonable means of attempting to correct the spinal deformity before the placement of internal fixation devices. More aggressive surgical treatment is recommended for patients with progressive myelopathy resulting from dynamic instability 2.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.