
Presentation
Dull, aching, intermittent pelvic pain with regular menses.
Patient Data
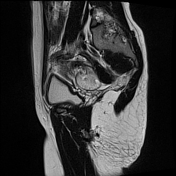


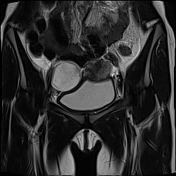
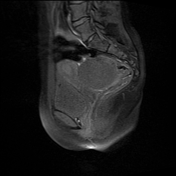
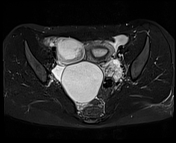
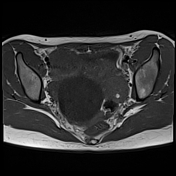

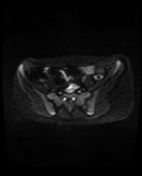
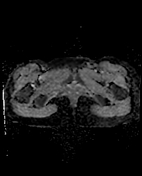
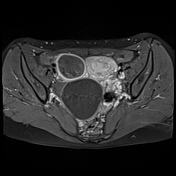
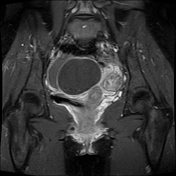
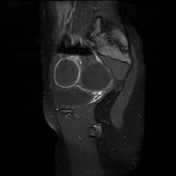
An enlarged left ovary, measuring about 2.8 x 3.8 x 3.35 cm in axial and craniocaudal dimensions with volume = 17 cc. It elicits predominant low T1, heterogenous bright T2, STIR, and mild restricted diffusion. It shows peripherally arranged follicles resembling a string of pearls. One of the follicles elicits a high T1 (haemorrhagic signal) with a perifollicular low T2 signal. It shows scanty heterogeneous post-contrast enhancement.
An oedematous, heterogeneous tube-like structure lies between the uterus and the left ovary, indicating a twisted pedicle and left fallopian tube, characteristic of a whirlpool sign.
A large midline left para-ovarian cyst is being inseparable from the left ovary (predisposing lead of the twist).
The uterus appears to be pulled to the left of the midline towards the side of the affected ovary (uterine tilting) as the twisted ovary pulls the uterus by the utero-ovarian ligament.
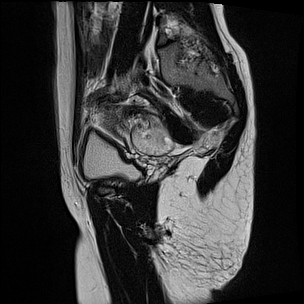
A right ovarian cyst shows a low T1 signal and a slightly heterogeneous high T2 and STIR signals with no restricted diffusion. It exhibits marginal post-contrast enhancement, with splayed ovarian tissue adjacent to the cyst.
There are mild pelvic ascites.
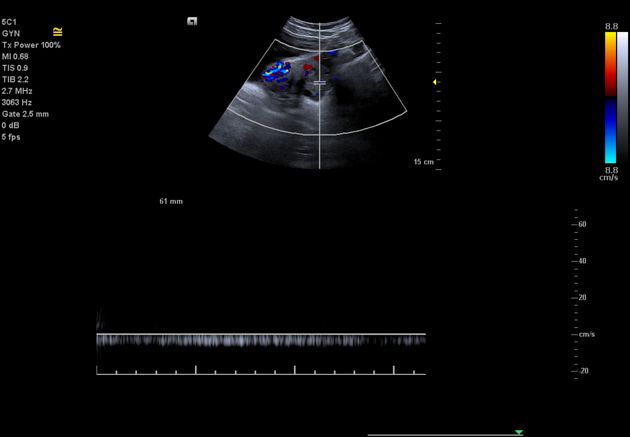
The ultrasound and Doppler findings were:
an enlarged left ovary with a twisted vascular pedicle showing preserved vascularity
the left ovarian parenchyma showed low but preserved arterial with a high-resistant waveform pattern and preserved venous waveforms
large pelvic midline left para-ovarian clear cyst
the right ovary was also enlarged showing a large cyst with a heterogenous internal echogenicity and posterior acoustic enhancement as well as no internal vascularity, likely complicated versus haemorrhagic cyst. The ovarian stroma showed preserved arterial and venous vascularity
Case Discussion
In this case, the predisposing factor for ovarian torsion was the presence of a large para-ovarian cyst connected to the left ovary. Intermittent chronic dull pain suggests chronic torsion/detorsion.
In this case, the imaging features of ovarian torsion are:
asymmetric ovarian enlargement
oedematous stroma
peripherally located follicles (string of pearls)
adjacent free fluid
foci of stromal haemorrhage
whirlpool sign (twisted vascular pedicle)
abnormal ovarian location
uterine tilting
A peri-follicular T2-hypointense rim sign on MRI in our case suggests the presence of perifollicular haemorrhagic changes.
Doppler features of ovarian torsion can include high-resistance arterial waveforms, followed by loss of venous flow and worsening oedema, leading to further compromise in arterial inflow with resultant absent arterial waveforms.
In our case, modified arterial and venous flow in the pedicle were preserved with a high-resistance arterial waveform. The presence of colour Doppler flow and contrast enhancement on MRI suggests that the affected ovary is still viable but do not exclude the diagnosis of torsion.
Laparoscopy confirmed the diagnosis of left ovarian torsion; the left pedicle was untwisted and the para-ovarian cyst was removed.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.