
Presentation
Abdominal pain for two months before
Patient Data
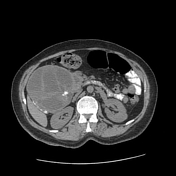




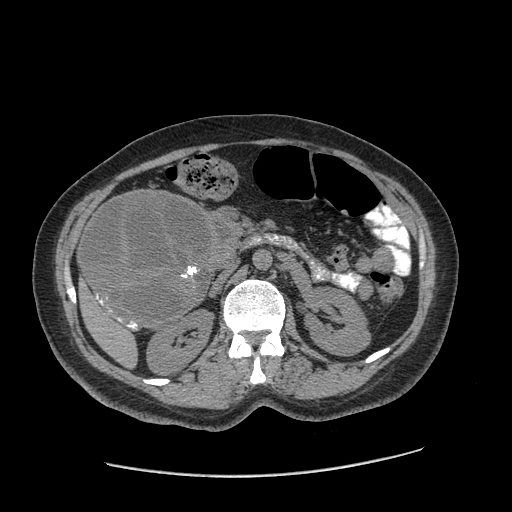
A large mass with prominent cystic components enhancing solid parts and calcified foci are seen in the pancreatic head with the widening of the duodenal C loop. The faint fluid-fluid level is visible on some cystic components. Hypervascularity, cystic components, and calcified foci are in favour of pancreatic neuroendocrine tumours.
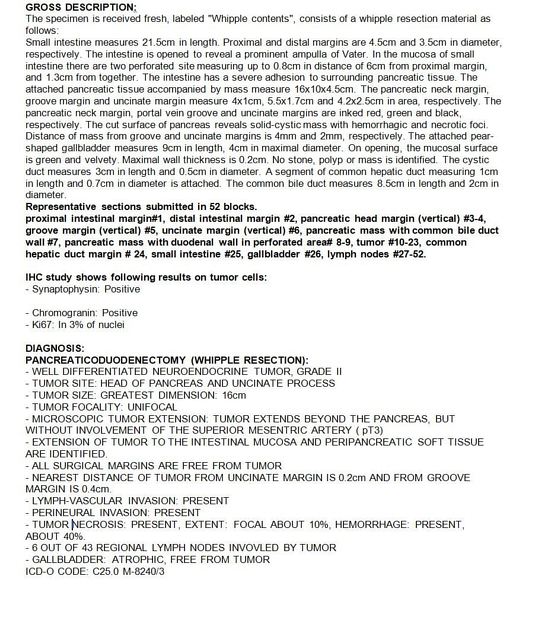
The photo of the pathology report shows that the tumour was a well-differentiated neuroendocrine tumour grade II.
Pathology
GROSS DESCRIPTION:
The specimen is received fresh, labelled “Whipple contents,” consists of a Whipple resection material as follows:
Small intestine measures 21.5 cm in length. Proximal and distal margins are 4.5 cm and 3.5 cm in diameter, respectively. The intestine is opened to reveal a prominent ampulla of Vater. In the mucosa of the small intestine, there are two perforated sites measuring up to 0 cm in distance of 6 cm from the proximal margin and 1.3 cm from each other. The intestine has severe adhesion to surrounding pancreatic tissue. The attached pancreatic tissue accompanied by the mass measures 16 x 10 x 4.5 cm. The pancreatic neck margin, groove margin, and uncinate margin measure 4 x 1 cm, 5.5 x 1.7 cm, and 4.2 x 2.5 cm in area, respectively. The pancreatic neck margin, portal vein groove, and uncinate margins are inked red, green, and black respectively. The cut surface of the pancreas reveals solid-cystic mass with haemorrhagic and necrotic foci. The distance of the mass from groove and uncinate margins is 1 mm and 2 mm, respectively. The attached pear-shaped gallbladder measures 9 cm in length, 4 cm in maximal diameter. On opening, the mucosal surface is green and velvety. Maximum wall thickness is 0.2 cm. No stone, polyp, or mass is identified. The cystic duct measures 3 cm in length and 0.5 cm in diameter. A segment of common hepatic duct measuring 1 cm in length and 0.7 cm in diameter is attached. The common bile duct measures 8.5 cm in length and 2 cm in diameter.
Representative sections submitted in 52 blocks:
Proximal intestinal margin (#1), distal intestinal margin (#2), pancreatic head margin (vertical) (#3-4), groove margin (vertical) (#5), uncinate margin (vertical) (#6), pancreatic mass with common bile duct wall (#7), pancreatic mass with duodenal wall in perforated area (#8-9), tumour (#10-23), common hepatic duct margin (#24), small intestine (#25), gallbladder (#26), lymph nodes (#27-52).
IHC study shows the following results on tumour cells:
Synaptophysin: Positive
Chromogranin: Positive
Ki67: In 3% of nuclei
Final Diagnosis
Well-differentiated neuroendocrine tumour, Grade II
Tumour site: Head of pancreas and uncinate process
Tumour size (greatest dimension): 16 cm
Tumour focality: Unifocal
Microscopic tumour extension: Tumour extends beyond the pancreas, but without involvement of the superior mesenteric artery (pT3). Extension of tumour to the intestinal mucosa and peripancreatic soft tissue are identified.
All surgical margins are free from the tumour.
Nearest distance of tumour from uncinate margin is 0.2 mm and from groove margin is 0.4 mm.
Lymph-vascular invasion: Present
Perineural invasion: Present
Tumour necrosis present, extent: Focal, about 10%; haemorrhage: Present, about 40%
6 out of 43 regional lymph nodes involved by tumour.
Gallbladder: Atrophic, free from tumour
Case Discussion
The patient underwent Whipple surgery and a well-differentiated grade II neuroendocrine tumour become confirmed. A pancreatic neuroendocrine tumour is in the differential diagnosis of cystic pancreatic masses.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}