
Presentation
Exercise intolerance and dyspnoea with recurrent pleural effusions
Patient Data

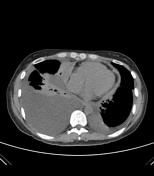


There is heterogeneously enhancing, diffuse, nodular pericardial thickening consistent with an infective/inflammatory pericarditis. The thickest pericardial rind measures 1.3 cm. The heart is not enlarged. Marked dilatation of the inferior vena cava is present despite the absence of cardiac chamber dilatation.
The liver demonstrates patchy heterogeneous enhancement which in addition to a dilated inferior vena cava is suggestive of passive liver congestion. Incidentally, dilated jugular veins are seen. These findings are suggestive of constrictive pericarditis.
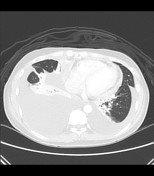
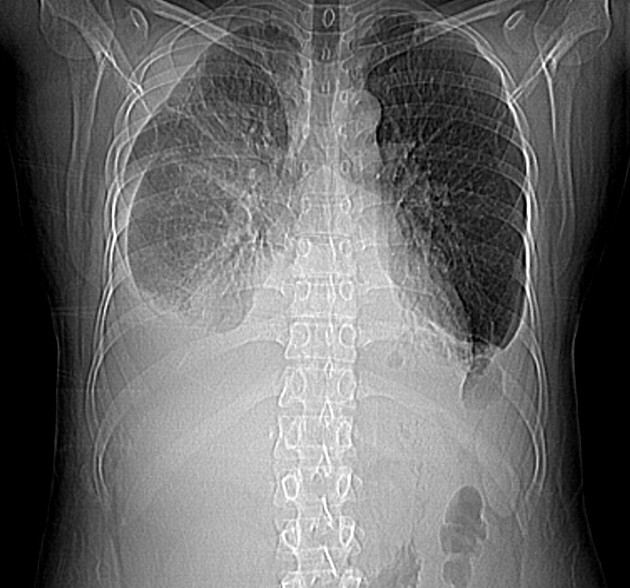
Bilateral pleural effusion, more in the right, and scattered areas of pleural thickening are demonstrated. There is atelectasis in the right middle and both lower lobes of the lungs. Fibrosis is seen in both upper lobes.
Multiple enlarged paratracheal, subaortic, subcarinal, prevascular and internal mammary lymph nodes are seen.
There is an aberrant right subclavian artery.
Case Discussion
This is a case of pericarditis diagnosed on computed tomography. Infection remains the most common cause of pericarditis, accounting for two-thirds of cases. Noninfectious causes account for one-third of cases.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.