
Presentation
Looks unwell. Presented with progressive throat pain, difficulty swallowing and hoarse voice. Pooling saliva in right pyriform fossa on endoscopy.
Patient Data
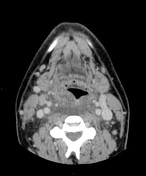

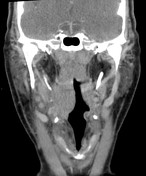

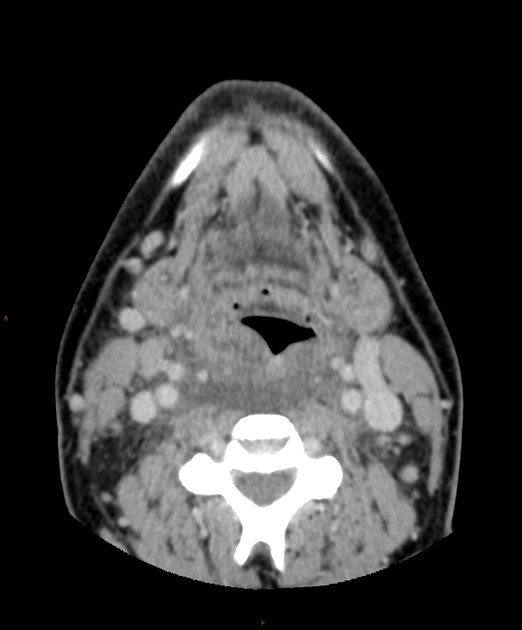
Diffuse pharyngeal mucosal space oedema, particularly right sided with thickening and elevation of the mucosa in the oropharynx, but no airway compromise.
Retropharyngeal fluid extending from C3 to the proximal oesophagus (best seen on sagittal reformat); but no defined enhancing wall. Inflammatory stranding in both carotid spaces and spreading down the anterior cervical tissues.
Reactive lymph node appearances, but no focal concerning features. Major vessels remain patent. Normal included intracranial structures.

Fine stranding and trace free fluid in the upper mediastinal fat adjacent to the oesophagus. This is compatible with mediastinitis, although again there is no abscess / collection.
Case Discussion
An example of airway infection / pharyngitis complicated with spread into the deep neck spaces, namely into the retropharyngeal space which can act as conduit of infection to spread into the mediastinum. This florid example also shows inflammatory change in the anterior cervical tissues which is a common and easier route of infection.
Our centre uses a 100 second delay for CT necks. However, to help differentiate between phlegmon and abscess either a repeat examination after a few minutes or diffusion MRI sequences can be useful.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.