
Presentation
Facial and right-hand numbness, CT demonstrated an abnormality. MRI for further assessment.
Patient Data
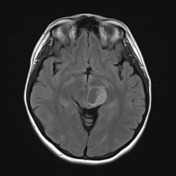


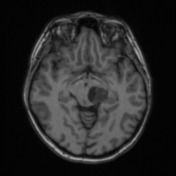
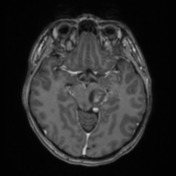
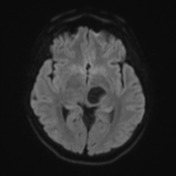
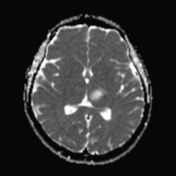
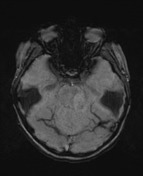
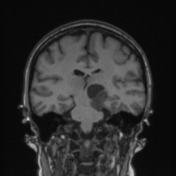
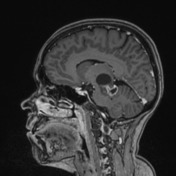
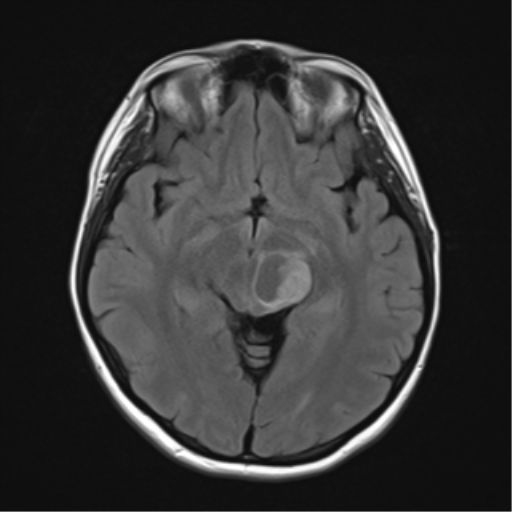
A mixed solid and cystic tumour is present, arising from the left side of the midbrain, with the cyst projecting superiorly displacing the left thalamus and third ventricle, and inferiorly prolapses out of the brain stem into the ambient cistern and more inferiorly into the cerebellopontine angle abutting and displacing the middle cerebral peduncle.
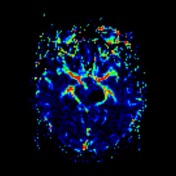
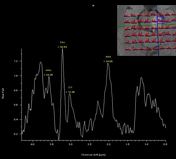
There is very little surrounding oedema, no calcification or blood product, and no elevation of cerebral blood volume. Spectroscopy demonstrates elevation of choline. The solid enhancing components demonstrate intermediate diffusion restriction (1400 x 10^-6 mm^2/s).
The remainder of the brain is unremarkable, there is no hydrocephalus. No other lesions identified.
Conclusion: Mixed solid cystic tumour arising from the left side of the midbrain and extending into the ambient cistern and cerebellopontine angle most likely represents a pilocytic astrocytoma.
Case Discussion
The patient went on to have a resection.
Histology
Sections show fragments of a moderately cellular glial tumour with mostly fibrillar and some microcystic areas. Tumour cells have round global nuclei with finely granular chromatin and focal bipolar processes. Rosenthal fibres and eosinophilic granular bodies are present. There is focal glomuerloid vascular proliferation. There is no necrosis. Multinucleated cells with smudgy degenerative type chromatin are present in a few areas. There is no normal parenchyma seen. Mitoses are few.
Immunohistochemistry results show tumour cells stain:
- GFAP Positive
- IDH-1 R132H Negative (not mutated)
- ATRX Positive (not mutated)
- p53 Mixed (not mutated)
- p16 CDKN2A Mixed (not mutated)
- Topoisomerase labelling index: 5%
- Synaptophysin is weakly positive.
Final diagnosis: pilocytic astrocytoma.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.